Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
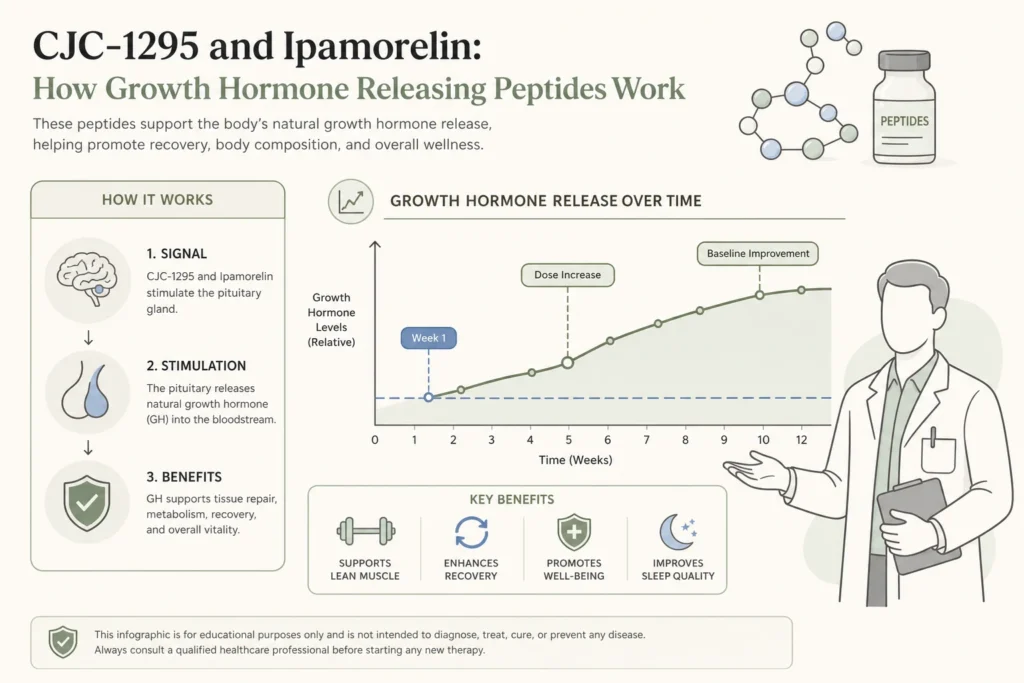
The CJC-1295 ipamorelin combination has become the default stack in physician-supervised peptide programs, and for good reason. The pairing lines up with how the body actually makes growth hormone, with one peptide raising the baseline tone of growth hormone release and the other producing the natural pulse. The biology is more elegant than social media hype suggests, and the realistic outcomes are more measured than the marketing.
This guide explains what each peptide does at the receptor level, why providers combine them, what to expect for body composition, sleep, and recovery, how this approach differs from synthetic human growth hormone, and how Body Works evaluates candidates in Franklin, TN and Nolensville, TN. The focus throughout is the mechanism the combination is designed to mimic and the honest limits of what a peptide protocol can do.
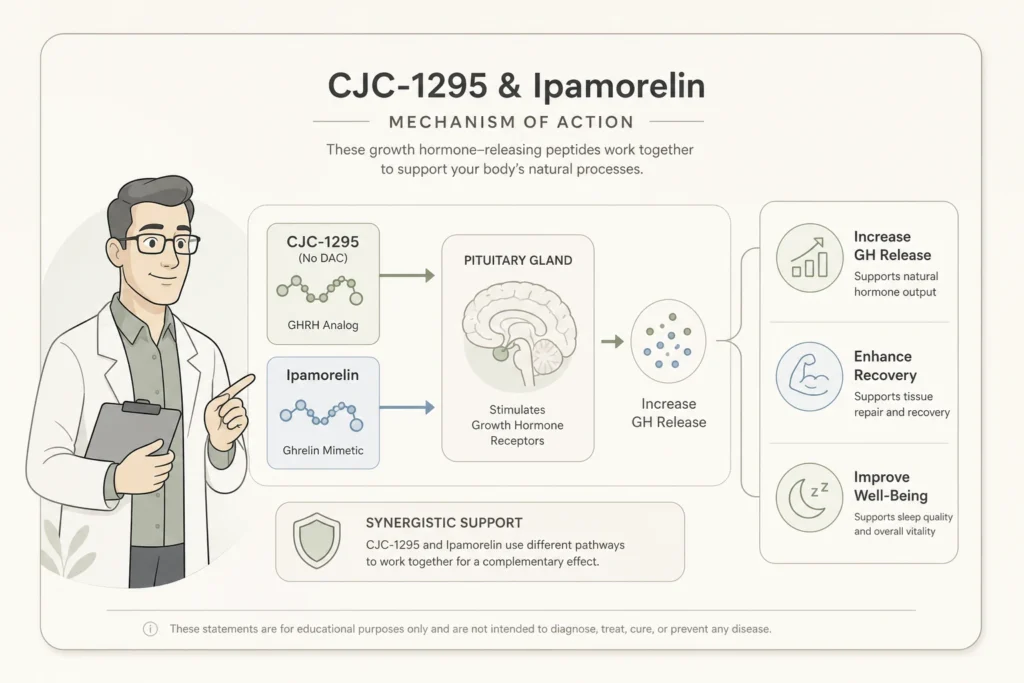
CJC-1295 is a synthetic analog of growth hormone releasing hormone, the natural signal the hypothalamus uses to tell the pituitary gland to release growth hormone. The peptide binds the same receptor on pituitary somatotroph cells that the body’s own GHRH binds, and it triggers the same downstream release of growth hormone. The chemistry is engineered for a longer half-life than native GHRH, which lasts only minutes in circulation, so a single dose extends the GHRH signal across hours or days depending on the formulation.
The original human pharmacology was characterized by Teichman et al., prolonged stimulation of GH and IGF-I secretion, Journal of Clinical Endocrinology and Metabolism, 2006. That study reported dose-dependent increases in plasma growth hormone of two to ten times baseline lasting six days or more after a single injection, with parallel rises in IGF-1 of one and a half to three times baseline. The signal is steady, not spiking, which matters for how the rest of the endocrine system responds.
Ipamorelin is a small synthetic peptide that mimics ghrelin, the hunger hormone made in the stomach. Ghrelin has a second, less obvious job beyond appetite: it binds the growth hormone secretagogue receptor in the pituitary and triggers a sharp pulse of growth hormone release. Ipamorelin keeps the growth hormone part of that signal and discards the rest, which is what makes it useful clinically. Older growth hormone releasing peptides like GHRP-2 and GHRP-6 also raised cortisol, prolactin, and ACTH at higher doses. Ipamorelin does not.
The original selectivity work was reported by Raun et al., the first selective growth hormone secretagogue, European Journal of Endocrinology, 1998. Researchers showed that even at doses more than 200 times the level needed to release growth hormone, ipamorelin did not significantly raise cortisol or ACTH compared with placebo. That clean profile is the reason ipamorelin became the preferred ghrelin mimetic for adult wellness protocols and why it is now the partner of choice for CJC-1295.
The pairing exists because the two peptides act on two different receptors that produce two different kinds of growth hormone release. CJC-1295 raises the baseline tone of GH release through the GHRH receptor. Ipamorelin produces a sharp pulse through the ghrelin receptor. Combining them produces a higher peak and a larger area under the curve than either peptide alone, while keeping the rhythm pulsatile rather than constant. That rhythm matters because the body’s own growth hormone system is pulsatile by design, and steady elevation is associated with insulin resistance, fluid retention, and tissue overgrowth.
A clinical review by Sigalos and Pastuszak on the safety and efficacy of growth hormone secretagogues in Sexual Medicine Reviews, 2017 describes GHRH analogs and ghrelin mimetics working together to raise growth hormone release more than either does alone, with limited adverse events reported across the published trials. The review is honest about the caveats. Most studies are short, sample sizes are modest, and long-term outcome data is still thin.
Synthetic human growth hormone is the hormone itself, manufactured in a lab and injected directly. The body sees a flood of exogenous growth hormone that bypasses the pituitary entirely, suppresses the body’s own production through normal feedback loops, and runs whether the body needs it or not. Growth hormone releasing peptides work upstream. They prompt the pituitary to release its own growth hormone in the patient’s native pulsatile rhythm, and the body’s own feedback systems remain in the loop.
This is the central reason regenerative medicine clinicians prefer the peptide approach for adult wellness in patients without diagnosed pituitary disease. According to Cleveland Clinic patient education on human growth hormone, recombinant HGH is a prescription therapy reserved for diagnosed growth hormone deficiency, certain pediatric short-stature conditions, and a small set of approved adult indications. For everyone outside those approved categories, the peptide pathway is the lane that respects the body’s existing endocrine rhythm. A deeper side-by-side comparison lives in the comparison of peptides versus HGH.
The honest answer is gradual and dose-dependent. Most supervised protocols target three primary outcomes: improved body composition with modest fat loss and lean mass retention, better sleep quality with longer slow-wave phases, and faster recovery from training or injury. Patients on a well-structured protocol often describe deeper sleep within the first two to four weeks, recovery improvements across four to eight weeks, and body composition shifts that build over three to six months when paired with consistent training and nutrition.
The realistic framing matters. Growth hormone is one input into body composition, not the dominant one, and patients who expect the kind of changes seen in studies of frank growth hormone deficiency will be disappointed. Endocrine Society clinical practice guidance on adult growth hormone deficiency emphasizes that the meaningful benefits in randomized trials are concentrated in patients with diagnosed deficiency, and that wellness-range users should expect smaller, slower changes. For a detailed timeline broken out by goal, see the article on peptide therapy timelines.
Safety in the published literature has looked favorable when these peptides are used in healthy adults at standard physician-supervised doses. The most common reported effects are injection site reactions, transient flushing or tingling shortly after administration, and mild water retention in some users. Insulin resistance has been reported with higher cumulative doses or with the long-acting CJC-1295 with DAC variant, which raises growth hormone tone continuously. Sleep architecture changes are usually the patient’s first felt signal, often within the first few weeks.
Candidacy matters. Patients with active malignancy or a personal history of cancer should not pursue growth hormone secretagogues without specialist input, because growth hormone signaling intersects with cell proliferation pathways. Pregnant or breastfeeding patients are not candidates. Patients with diabetes, especially poorly controlled diabetes, need careful evaluation because of the insulin sensitivity question. Patients with active pituitary pathology require an endocrinology evaluation rather than a peptide protocol. These contraindications are part of why provider selection matters, and the article on choosing a peptide therapy provider covers the questions to ask.
The patients who do best with CJC-1295 plus ipamorelin tend to be healthy adults in their 30s to 60s with realistic goals around recovery, body composition, sleep, or general regenerative support, who have already covered the basics of training, sleep, and nutrition. Men on testosterone replacement therapy sometimes benefit from the addition of a growth hormone peptide because the two endocrine systems interact, and the men’s hormone therapy program at Body Works is the right entry point for that combined plan. Patients chasing peptide therapy because nothing else has worked are usually not the right fit until the underlying lifestyle factors are addressed.
The evaluation at Body Works starts with a consultation, a review of medical history and current medications, and bloodwork including IGF-1 when clinically indicated. If the combination is appropriate, the protocol is built around the patient’s specific goals, with a sleep-focused primer phase often coming first because better sleep is the earliest signal most patients feel. Patients who want to read more on the sleep angle can see the dedicated piece on growth hormone peptides and sleep recovery, and the broader framework lives in the complete guide to peptide therapy.
The right next step is a consultation with a physician who works with this category, not a checkout page from an online vendor. Growth hormone releasing peptides are prescription compounds dispensed through accredited 503A compounding pharmacies, and the dosing, scheduling, and follow-up that produce good outcomes require a clinical relationship. A physician-supervised regenerative peptide therapy program at Body Works in Franklin and Nolensville handles the candidacy review, sourcing, dosing, and monitoring that the published literature recommends.
If recovery, sleep, or body composition has you researching peptides, the most useful thing you can do is talk to the team. Schedule a Free Consultation with Body Works. You can reach the Franklin office at (615) 790-2548 or the Nolensville office at (615) 941-1000.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
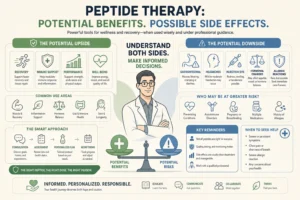
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never