Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the deep belly fat that sits around your organs. That is the promise attached to tesamorelin, and unlike most peptide marketing, it is rooted in real clinical trials. When researchers tested tesamorelin visceral fat reduction in a study of 412 patients, the deep abdominal fat dropped by 15.2 percent in six months while the placebo group actually gained fat.
That headline number is impressive, and it is also where the conversation usually stops. The full story has more to it. Tesamorelin is a prescription medication with a specific FDA-approved use, a defined mechanism, real limits, and a safety profile that demands lab monitoring. It is not a shortcut, and it is not the same thing as a GLP-1 weight loss medication, even though both can change how your body looks.
This article walks through how tesamorelin works, what the evidence does and does not prove, how it compares to other body composition peptides, and who is actually a candidate. At Body Works, every peptide protocol starts with a physician, bloodwork, and a clear reason for treatment, not a trend.
Tesamorelin works by signaling your own pituitary gland to release more growth hormone, which in turn raises insulin-like growth factor 1 (IGF-1) and triggers the breakdown of stored fat. It is a synthetic analog of growth hormone-releasing hormone (GHRH), a 44-amino-acid peptide modified so it resists rapid breakdown in the bloodstream. Rather than injecting growth hormone directly, tesamorelin nudges your endocrine system to make more of its own.
This distinction matters. Because the body still controls the final release through its normal feedback loops, the rise in growth hormone is more physiologic than flooding the system with synthetic hormone. The downstream effect is increased lipolysis, the mobilization of fat for energy, with a notable preference for visceral adipose tissue.
A review of tesamorelin in HIV-associated lipodystrophy published in HIV/AIDS (Auckland) describes it as a stabilized GHRH analog that stimulates endogenous growth hormone secretion and raises IGF-1, producing a selective reduction in visceral fat. That selectivity for deep abdominal fat, rather than the fat just under the skin, is what made it interesting to researchers in the first place.
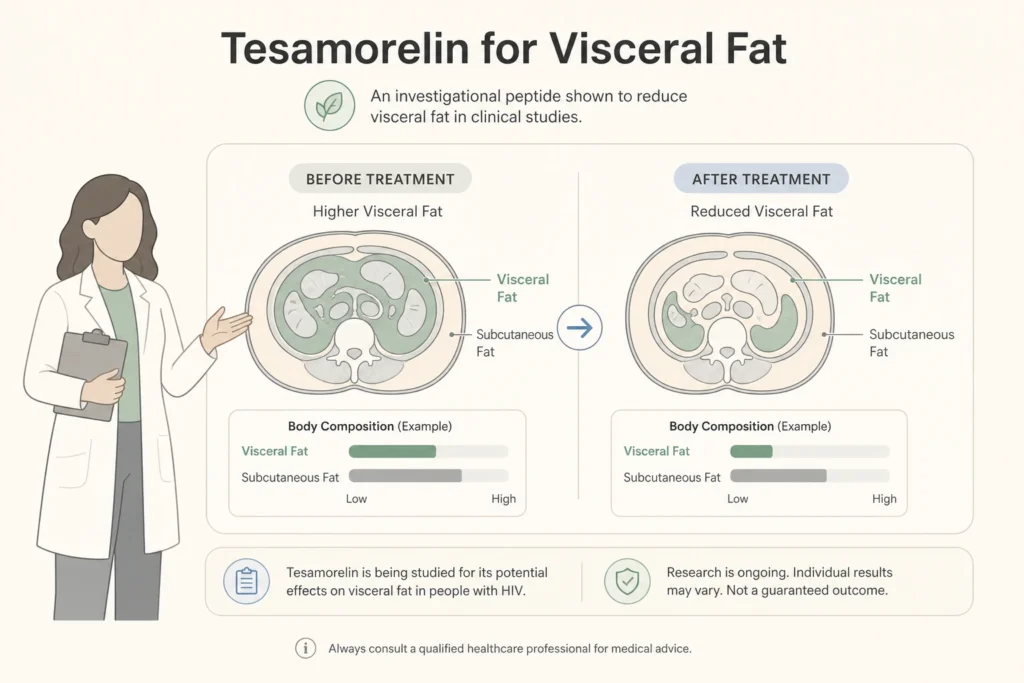
Visceral fat is the fat stored deep in the abdomen, wrapped around the liver, intestines, and other organs, and it behaves very differently from the soft fat you can pinch at your waist. Subcutaneous fat sits under the skin and is largely a storage and cushioning tissue. Visceral fat is metabolically active, releasing inflammatory signals and free fatty acids that are linked to insulin resistance, abnormal cholesterol, and cardiovascular risk.
This is why a peptide that selectively targets visceral fat drew clinical attention. Reducing deep abdominal fat is associated with measurable metabolic improvement, not just a flatter midsection.
In a 2012 analysis published in Clinical Infectious Diseases on visceral adiposity and metabolic profile, patients who lost 8 percent or more of their visceral fat on tesamorelin showed significantly better triglyceride and glucose outcomes than those who did not respond. The takeaway is that where you lose fat can matter as much as how much you lose, and visceral fat is the compartment most tied to metabolic health, so reducing it carries weight beyond appearance.
The strongest evidence for tesamorelin comes from large randomized trials in HIV patients with lipodystrophy, where it consistently reduced visceral fat without disrupting blood sugar. In the landmark phase 3 study, the medication produced a clear and selective drop in deep abdominal fat compared to placebo over six months.
According to a 2007 randomized controlled trial in the New England Journal of Medicine, visceral adipose tissue decreased by 15.2 percent in the tesamorelin group while increasing by 5.0 percent in the placebo group over 26 weeks, alongside improvements in triglycerides and cholesterol ratios, with no significant adverse effect on glucose control. A separate placebo-controlled trial with a safety extension reported a 10.9 percent reduction in visceral fat and a rise in IGF-1 without glucose perturbation.
The limits are just as important. Nearly all of this data comes from HIV-associated lipodystrophy, a specific condition, not from healthy adults seeking cosmetic fat loss. The reviews also note that the visceral fat returns toward baseline once treatment stops, meaning the effect is maintained only while the medication continues. Tesamorelin is studied, but it is studied in a narrow population.
Tesamorelin, AOD-9604, and GLP-1 medications all influence body composition, but they act through completely different pathways and have very different evidence behind them. Tesamorelin raises your own growth hormone to mobilize visceral fat. AOD-9604 is a fragment of the growth hormone molecule marketed for fat loss, but it lacks the large human trial support that tesamorelin carries. GLP-1 medications such as semaglutide and tirzepatide work on appetite and blood sugar, driving total body weight loss rather than targeting one fat compartment.
| Factor | Tesamorelin | AOD-9604 | GLP-1 (semaglutide, tirzepatide) |
|---|---|---|---|
| Primary mechanism | Raises endogenous growth hormone and IGF-1 | Growth hormone fragment, claimed lipolytic effect | Appetite suppression and glucose regulation |
| Main effect | Selective visceral fat reduction | General fat loss (limited human data) | Significant total body weight loss |
| FDA status | Approved for HIV lipodystrophy | Not FDA approved for weight loss | Approved for weight management and diabetes |
| Strength of evidence | Multiple large randomized trials | Weak, mostly preclinical | Large randomized trials |
If your goal is total body weight loss, a GLP-1 protocol is the more evidence-backed path, and some people combine strategies under supervision. Our guide on how peptides and GLP-1 weight loss fit together explains where these approaches overlap and where they do not, and our medical weight loss program can help you choose.
A genuine candidate for tesamorelin is someone with a documented medical reason for treatment, normal or monitored growth hormone status, and no contraindications, evaluated by a physician. The on-label population is adults with HIV-associated lipodystrophy and excess abdominal fat. Any use outside that, sometimes discussed for stubborn visceral fat or metabolic concerns, is off-label and should only happen under careful medical oversight.
Tesamorelin is not appropriate for everyone. It is contraindicated in pregnancy, in people with active cancer, and in those with disorders of the pituitary gland or certain pituitary tumors, since stimulating growth hormone could be harmful in those settings. Because it raises IGF-1, candidacy always involves bloodwork before and during treatment.
Per the LiverTox tesamorelin monograph from the National Institutes of Health, the medication raises IGF-1 levels and monitoring for elevations during therapy is recommended. This is not a peptide to source online and self-administer; it is a prescription with real eligibility criteria. Curious where peptides fit into a broader plan? Start with our complete guide to peptide therapy.
Physician supervision with regular bloodwork is essential for tesamorelin because the medication works by raising hormones that must stay within a safe range. The same IGF-1 elevation that helps mobilize visceral fat can, if unmonitored, push hormone levels higher than intended, which is why baseline and follow-up labs are standard practice.
According to the FDA prescribing information for tesamorelin, the medication is indicated for the reduction of excess abdominal fat in HIV-infected patients with lipodystrophy, and the label directs clinicians to monitor IGF-1 and assess for glucose intolerance during treatment. A supervised protocol also screens for the contraindications that matter, tracks response, and stops treatment if the risk outweighs the benefit.
This is the same standard we apply to every growth hormone peptide, including pairs like CJC-1295 and ipamorelin, and repair-focused peptides such as BPC-157 for tissue recovery. The peptide is only one part of the plan; the labs, the physician, and the follow-up are what make it responsible care rather than a gamble.
Tesamorelin sits at the intersection of strong science and narrow indications, which is exactly why it deserves a real conversation rather than a quick online order. For the right person with a clear medical reason and proper monitoring, it is a well-studied tool. For someone simply chasing general weight loss, a GLP-1 protocol or a structured metabolic program is usually the better fit.
At Body Works, peptide decisions are made by a physician after reviewing your goals, your history, and your bloodwork, never from a template. We serve patients in Franklin, TN and Nolensville, TN, and our peptide therapy program is built around supervised, lab-guided care.
If you want to know whether a body composition peptide makes sense for you, or whether a different approach fits your goals better, the next step is a conversation with our team. Schedule a Free Consultation to review your options with a physician. Our offices in Franklin and Nolensville make it easy to get started close to home.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never
“Weeks to months.” That is the answer almost every peptide therapy provider hands a patient who asks how long it takes to feel something. It