Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
Hair shedding ranks consistently among the top concerns patients raise before starting Body Works semaglutide therapy program or tirzepatide. Search volume on “does semaglutide cause hair loss” has climbed in lockstep with the medications themselves, and dermatology clinics across the country report a steady stream of questions from GLP-1 patients worried that their treatment is damaging their hair.
The honest answer is that hair shedding does happen for some patients on GLP-1 medications, but the cause is rarely the drug itself. The shedding pattern, the timing, and the resolution all match a well-described condition called telogen effluvium, which is triggered by rapid weight loss regardless of how the loss happened. Understanding the mechanism, the timeline, and the strategies that reduce the risk turns this from a frightening side effect into a manageable, often preventable, part of treatment.
This guide walks through what the clinical evidence shows, when shedding typically starts and stops, and what a physician-supervised medical weight loss program can do to reduce the risk for patients who are already worried about their hair before they start.
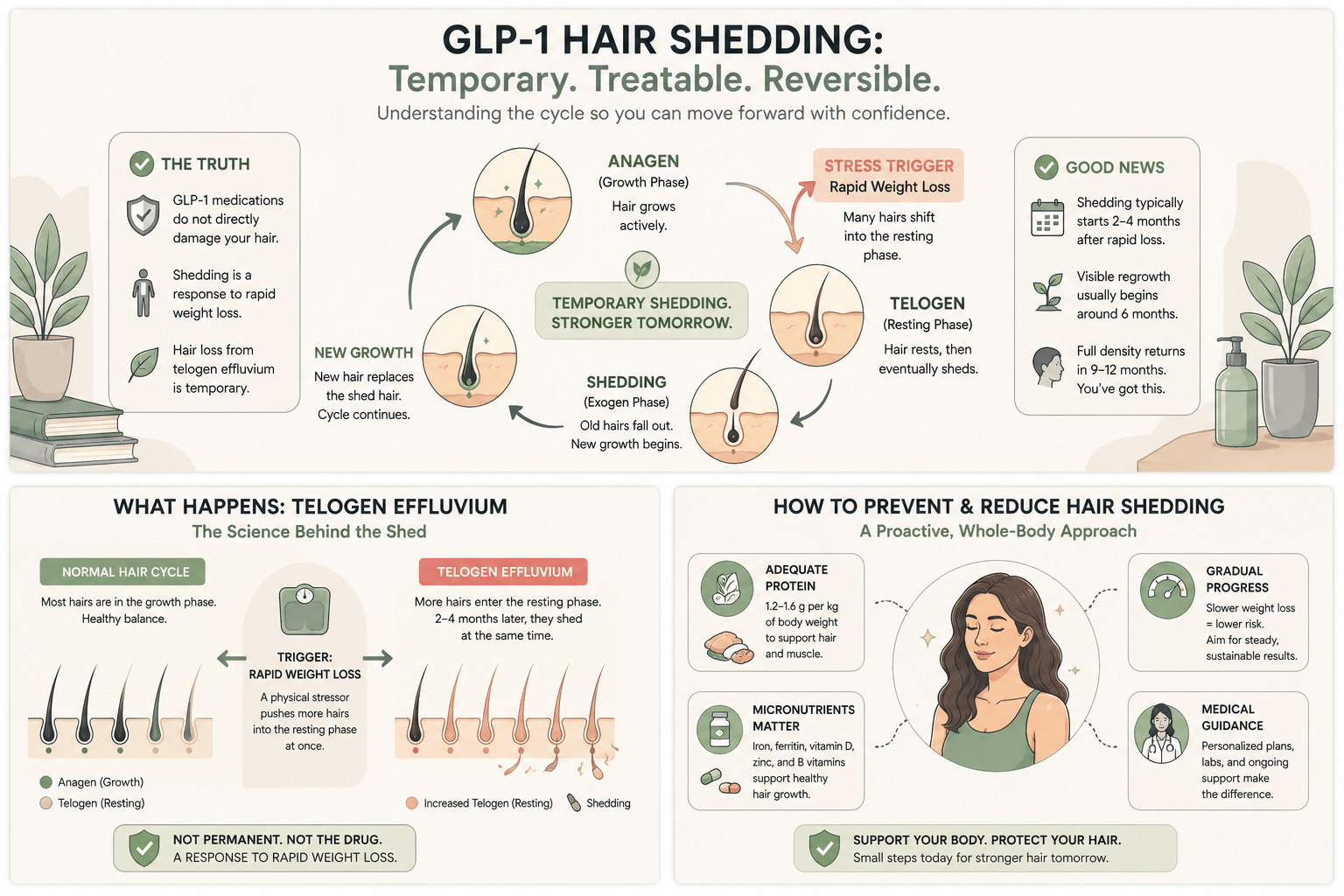
The hair on your head is in one of three phases at any given moment: anagen (growing), catagen (transitioning), or telogen (resting and shedding). On a normal day, about 85 to 90% of your hair is in anagen, and you shed roughly 50 to 100 hairs as old telogen hairs are pushed out by new anagen growth.
Telogen effluvium is what happens when a stressor pushes a much larger share of hair into the telogen phase at the same time. Two to four months after the trigger, those hairs all reach the end of telogen and shed in a synchronized wave. Patients notice clumps in the shower, increased thinning at the part line, and a temporary visible reduction in density. The condition is not permanent. New anagen hairs replace the shed ones over the following six to nine months, and the hair density typically returns to baseline (American Academy of Dermatology).
Rapid weight loss is one of the most common triggers of telogen effluvium, and this is true whether the loss comes from bariatric surgery, very-low-calorie diets, severe illness, or GLP-1 medications. The medication is not directly attacking your hair follicles. The medication is producing rapid loss, and rapid loss is what the follicles are responding to.
In the STEP 1 trial of semaglutide 2.4 mg, hair loss was reported by 3.0% of participants compared to 1.0% on placebo, a clinically modest but real difference (Wilding et al., New England Journal of Medicine, 2021). Tirzepatide trials report hair shedding at a similar single-digit rate. Real-world rates may be higher than trial rates because patients in clinical practice often lose weight faster than the average trial participant, and faster loss correlates with stronger telogen effluvium signal.
The pattern is more common in women than in men, partly because women are more likely to notice and report the change and partly because diffuse thinning is more visible in longer hairstyles. Patients with a personal or family history of any pattern of hair thinning may also experience telogen effluvium that unmasks an underlying tendency, with regrowth coming back at slightly lower density than before.
Hair shedding rates on GLP-1 medications are lower than the rates seen after bariatric surgery, where 30 to 40% of patients report some hair loss in the first year. The mechanism is the same; the magnitude is smaller because GLP-1 weight loss is typically more gradual.
Telogen effluvium does not start the day you begin medication. The shedding wave usually appears two to four months after a substantial weight loss has occurred. For most semaglutide patients, this corresponds to month four through month seven of treatment, when titration has reached the therapeutic dose and the steepest part of the weight loss curve is happening.
The shedding lasts six to twelve weeks at its peak intensity. After that, new anagen growth pushes the shedding back to baseline rates. Visible regrowth, often as short fine hairs around the hairline and part, is detectable around six months after the shed begins. Full density recovery takes nine to twelve months from the shed onset.
If shedding has not begun to subside by month nine of treatment, or if it is accompanied by other unusual symptoms like scalp pain, redness, or patchy bald spots rather than diffuse thinning, the cause is likely something other than telogen effluvium and deserves a dermatology referral. Iron deficiency, thyroid dysfunction, autoimmune conditions, and androgenetic alopecia can all coincide with treatment and may need separate workup.
Several strategies, used together, meaningfully reduce the risk and severity of telogen effluvium during medical weight loss. None of them are exotic, and most are part of a well-built program already.
Adequate protein intake. Hair is largely keratin, a protein. Inadequate protein during a calorie deficit is a known telogen effluvium trigger independent of the medication. Most clinical guidelines recommend at least 1.2 to 1.6 grams of protein per kilogram of body weight per day during active weight loss, and on the higher end of that range for patients with hair shedding concerns. The same protein target also helps preserve muscle mass during GLP-1 treatment, which is the other reason it matters.
Iron and ferritin. Low ferritin is a common contributor to hair shedding in women, especially women of reproductive age. A baseline ferritin check is part of a thorough lab panel, and a ferritin below 50 ng/mL often warrants supplementation regardless of whether the patient is on a GLP-1.
Vitamin D, zinc, and biotin. Deficiencies in any of these can amplify shedding. A standard nutrition panel screens for them. Routine biotin supplementation in patients without a deficiency does not improve hair, despite the marketing claims.
Avoiding overly aggressive titration. Patients who push to higher doses faster than the standard schedule lose weight faster and trigger stronger telogen effluvium. Following the standard four-week titration interval, or extending it to six to eight weeks if tolerated weight loss is already brisk, reduces the magnitude of the shedding wave (FDA prescribing information for semaglutide).
Topical minoxidil, in selected patients. For patients with strong shedding or with an underlying tendency to thinning, low-strength topical minoxidil shortens the recovery time and supports the regrowth phase. This is a clinical decision that should be made with a provider, not a self-treatment.
Diffuse shedding that begins around month four, peaks for six to twelve weeks, and starts to taper is consistent with telogen effluvium and rarely requires intervention beyond the strategies above. Symptoms that fall outside that pattern deserve evaluation.
Bald patches rather than diffuse thinning suggest alopecia areata or another autoimmune cause. Scalp pain, burning, or redness suggests an inflammatory cause. Hair loss that worsens past month nine of treatment, or hair loss accompanied by fatigue, cold intolerance, or weight changes inconsistent with the treatment plan, suggests a thyroid or systemic cause that should be worked up. Hair loss with a clearly receding hairline rather than a diffuse part-line widening suggests androgenetic alopecia, which has its own treatment path.
None of these patterns are caused by the GLP-1 medication. They can occur during treatment by coincidence, and a provider can sort out which is which.
At Body Works, the conversation about hair starts at the initial consultation. Patients with a personal or family history of hair thinning are flagged for closer attention during titration. Lab work routinely includes ferritin, vitamin D, thyroid panel, and zinc, with supplementation guidance built into the plan when any of those run low.
Protein targets are individualized rather than recommended as a generic number, and the program supports patients with practical strategies for hitting them. For patients who experience shedding mid-treatment, a slightly slower titration, focused micronutrient support, and short-term topical interventions are all on the table. The goal is to deliver the weight loss without paying an unnecessary cost in hair.
Patients are also reminded that the shedding is temporary. Hair density returns. Knowing the timeline reduces the anxiety, and the right combination of nutritional support, paced titration, and patience produces both the weight loss and the regrowth on schedule. Schedule a free consultation to talk through how a personalized plan would handle this and other side-effect concerns.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never