Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The weight gain that arrives during perimenopause is genuinely different from weight gain at other times of life. It often shows up around the midsection where it was not before. It resists the diet and exercise approaches that worked at thirty-five. It tracks with sleep changes, mood shifts, and a metabolism that seems to have changed the rules without telling anyone. Patients in their forties and fifties describe it as fighting a different opponent, and they are not wrong.
GLP-1 medications have become a useful tool for many women navigating midlife weight gain, but the conversation around them often skips the parts that matter most for this population. Hormonal context shapes how the medication performs. Bone density, muscle mass, and cardiovascular risk all need closer attention in midlife than in earlier decades. Hormone therapy, if a patient is also using it, interacts with weight loss strategy in ways that should be explicit, not assumed.
This guide is for women in perimenopause or menopause considering whether physician-supervised semaglutide therapy or tirzepatide fits into a broader midlife health strategy. It covers the hormonal biology behind the weight pattern, what the evidence shows for GLP-1 effectiveness in this population, the side-effect questions that matter more after forty, and how a combined approach that addresses both hormones and metabolism produces better outcomes than either piece alone.
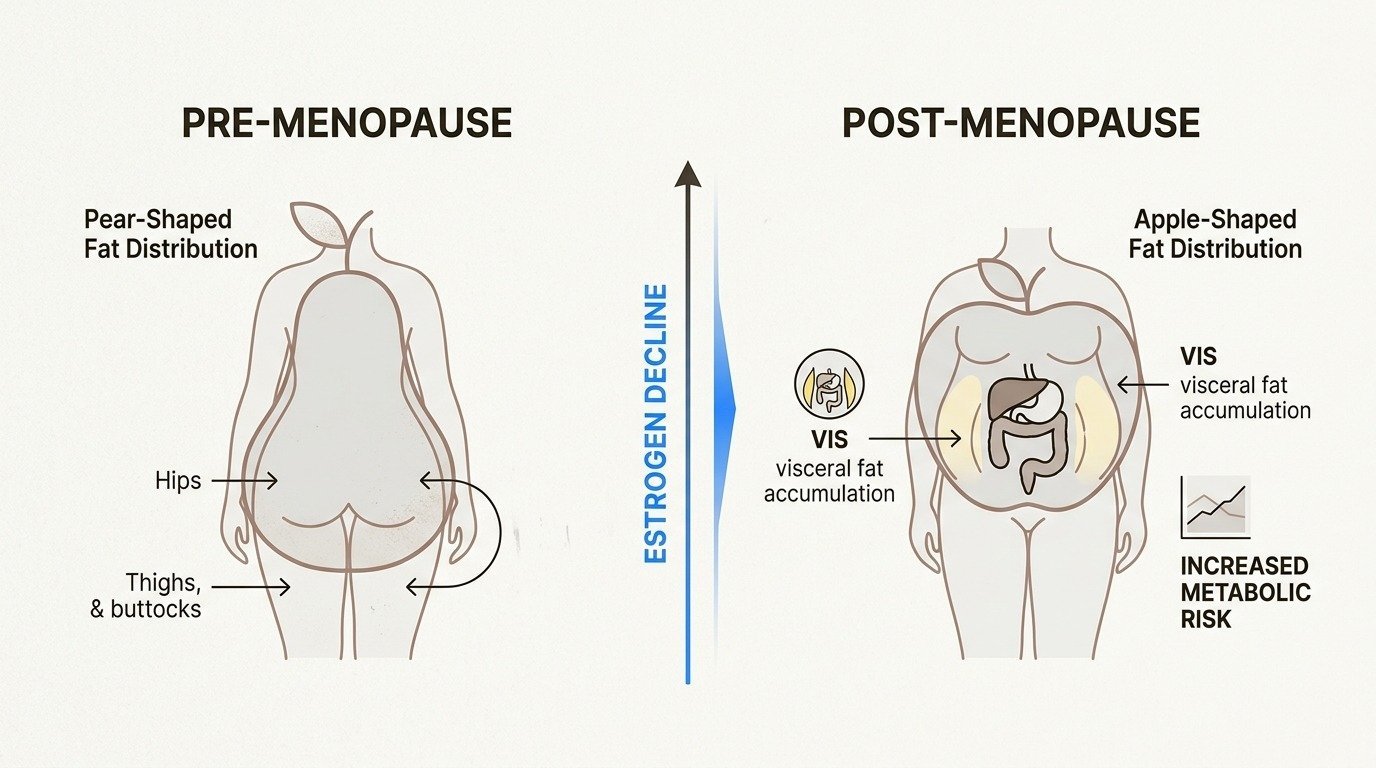
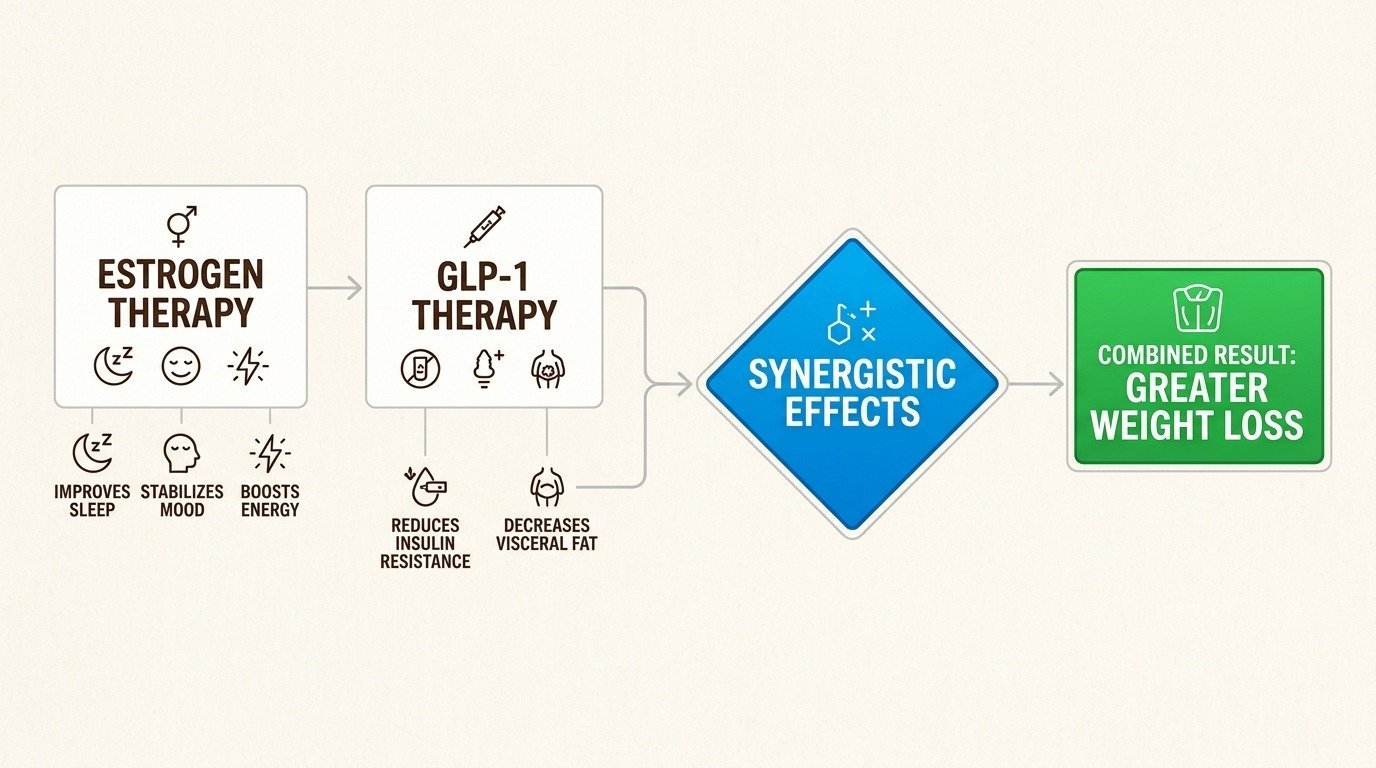
The weight pattern in midlife reflects a cluster of physiological changes happening at the same time. Estrogen levels begin to fluctuate during perimenopause, which can start as early as the late thirties for some women, and decline more steadily after menopause. Estrogen has direct effects on body composition: it influences where fat is stored, how the body processes carbohydrate, and the sensitivity of insulin signaling.
As estrogen declines, fat storage shifts from the hips and thighs to the abdomen. The midsection accumulation is not a cosmetic difference. Visceral fat, the fat surrounding internal organs, is metabolically active in ways that subcutaneous fat is not. It produces inflammatory signals, contributes to insulin resistance, and elevates cardiovascular risk. The metabolic profile of a midlife woman who has gained twenty pounds in the abdomen is meaningfully different from the metabolic profile of the same woman twenty pounds heavier at thirty.
At the same time, age-related muscle loss, called sarcopenia, accelerates after forty if not actively countered. Less muscle means a lower resting metabolic rate, which means the same eating pattern that maintained weight in the past now produces a slow gain. Sleep disruption from hot flashes and night sweats further dysregulates the appetite hormones leptin and ghrelin, increasing hunger and reducing fullness signals (North American Menopause Society on menopause and weight).
The cumulative effect is that midlife weight gain is multifactorial. Diet and exercise alone often produce smaller results than they did a decade earlier, not because effort is lower but because the physiology is different. This is the context in which GLP-1 medications become a clinically reasonable consideration.
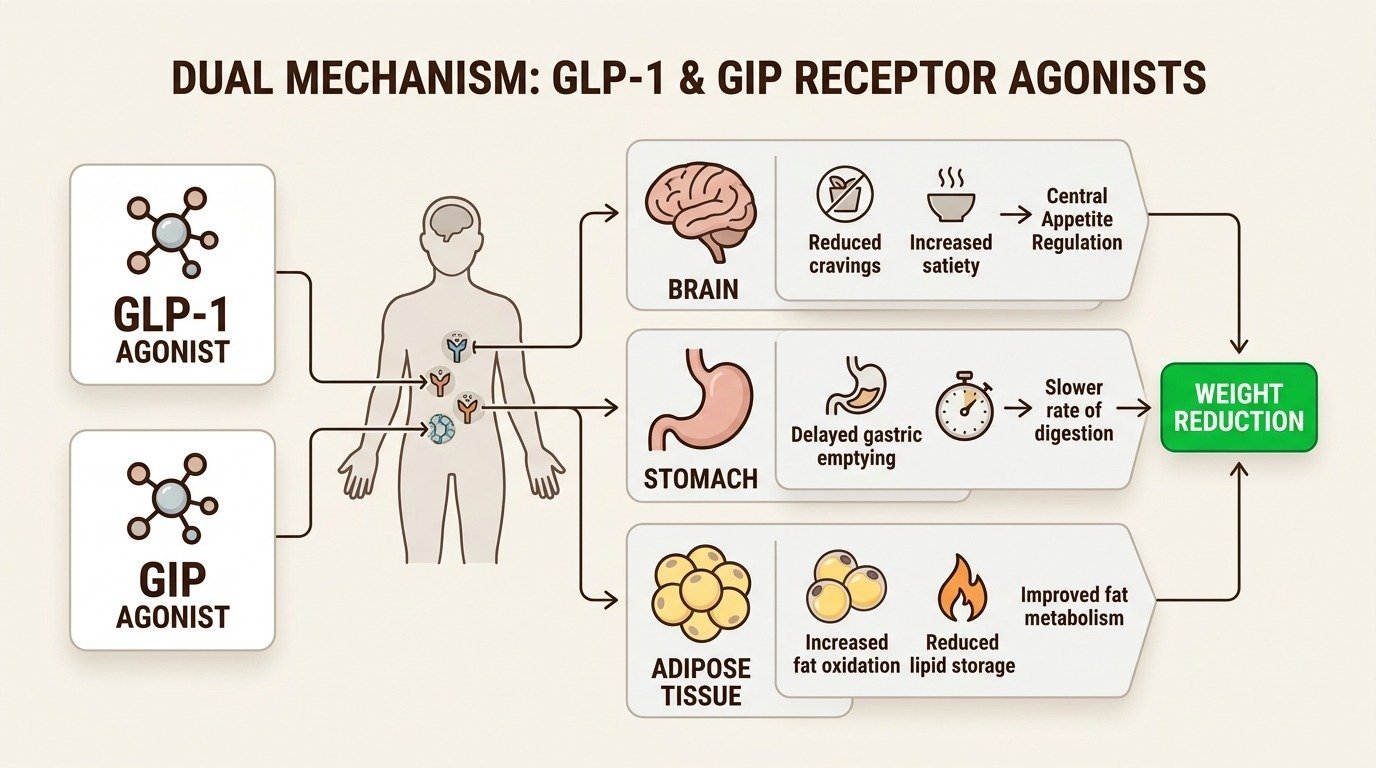
The major GLP-1 trials for weight management included substantial numbers of women in midlife, though they were not designed as menopause-specific studies. Subgroup analyses and follow-up research consistently show that women in the 45 to 65 age range respond to semaglutide and tirzepatide at rates similar to younger women, with average weight loss in the same 14 to 22 percent range depending on the medication and dose (Jastreboff et al., New England Journal of Medicine, 2022).
The weight loss tends to come disproportionately from visceral abdominal fat, which is the metabolically dangerous compartment. This means GLP-1 treatment in midlife often produces cardiovascular and metabolic benefits that exceed what the scale number alone suggests. Insulin sensitivity improves. Blood pressure often comes down. Lipid panels frequently shift in a favorable direction. For midlife women whose weight gain is intertwined with prediabetes, hypertension, or fatty liver, these secondary effects are sometimes more clinically meaningful than the weight number itself.
The medications are not magic. The weight loss is real, but it requires the same supporting infrastructure that any weight loss requires: adequate protein, resistance training to preserve muscle, sleep prioritization, and consistent follow-up. These elements matter more, not less, in midlife.
Many women in perimenopause and menopause are candidates for hormone therapy, which addresses estrogen and sometimes progesterone deficiency directly. Hormone therapy, when clinically appropriate, has its own effects on body composition. It modestly reduces abdominal fat accumulation, supports bone density, and improves the metabolic profile in ways that complement, rather than duplicate, what GLP-1 medications do.
Patients pursuing both interventions should be working with providers who understand both. Hormone therapy can change appetite patterns. GLP-1 medications can change how patients perceive hot flashes and other vasomotor symptoms. Lab work overlaps. The clinical conversation about cardiovascular risk, breast health, and venous thromboembolism risk all factor in. Coordinating both treatments under one clinical roof, or under tightly aligned providers, produces a cleaner protocol than running them in parallel through unconnected services.
Body Works provides both medical weight loss with GLP-1 medications and women’s hormone therapy. The clinical adjacency is one of the reasons the program is well suited to midlife patients. The same provider who prescribes the GLP-1 sees the hormone panel, knows the hot flash trajectory, and can build a single coherent plan rather than two parallel protocols.
The strongest evidence for this combined approach came in early 2026. A retrospective cohort study led by Mayo Clinic researchers, published in The Lancet Obstetrics, Gynaecology and Women’s Health, followed 120 postmenopausal women on tirzepatide for at least twelve months. Women who were also on systemic hormone therapy lost an average of 19.2 percent of their starting body weight, compared to 14.0 percent in women on tirzepatide alone (Castaneda et al., The Lancet Obstetrics, Gynaecology and Women’s Health, 2026). The share of women losing more than 20 percent of body weight was 45 percent in the hormone-therapy group, compared to 18 percent without it.
The study cannot prove causation because patients were not randomized. But the magnitude of the difference, and the consistency with the underlying biology, is large enough that midlife patients deserve to have hormone therapy explicitly discussed alongside any GLP-1 decision. The two treatments are not in competition. They appear to amplify each other.
Several side-effect considerations apply more strongly in midlife than in younger patients. Bone density is the most important. Rapid weight loss in any population can be associated with reduced bone mineral density, and postmenopausal women already face accelerated bone loss from estrogen decline. The protective strategy is identical to the protective strategy for muscle: adequate protein, vitamin D, calcium, and consistent resistance training. Patients with a personal or family history of osteoporosis warrant a baseline DEXA scan before starting an aggressive weight loss protocol.
Muscle preservation matters more in midlife because the baseline rate of sarcopenia is higher. Preserving muscle on GLP-1 medications in this age group requires deliberate attention to protein intake at the upper end of clinical recommendations and a non-negotiable resistance training component.
Hair changes, which are already common in midlife due to hormonal shifts, may overlap with the temporary telogen effluvium associated with rapid weight loss. The combination can be more visible than either cause alone. Recognizing the dual contribution helps avoid attributing all of it to the medication when hormones are also a factor.
Cardiovascular risk monitoring is also worth attention. Most midlife women on GLP-1 medications see favorable cardiovascular markers over time, but baseline assessment, including a lipid panel, blood pressure tracking, and consideration of HbA1c, gives the provider the data needed to identify a problem early if one emerges.
The general candidacy questions for GLP-1 medications apply in midlife, with a few modifications. The standard threshold is a BMI of 30 or higher, or a BMI of 27 or higher with weight-related comorbidities. Comorbidities are more common in midlife, so more women in the 27 to 30 BMI range qualify on the comorbidity criterion than they might have understood.
Patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 are not candidates. Patients with active gallbladder disease, pancreatitis, or severe gastroparesis warrant a careful clinical evaluation before starting. Patients on certain other medications may need dose adjustments or monitoring changes.
The broader fit question, beyond the medical criteria, is whether the patient is positioned to add the supporting work that makes the medication effective. Resistance training, protein focus, sleep prioritization, and stress management are not optional add-ons in midlife. They are part of the protocol. A patient who is able to build those elements into the plan is positioned for excellent outcomes. A patient who is not is better served by addressing those foundations first and revisiting medication later. Our broader candidacy guide for who is a good candidate for semaglutide covers the medical criteria in more depth.
Patients in midlife who come to Body Works typically receive a more integrated initial assessment than patients in other age groups. Lab work includes a full thyroid panel, comprehensive metabolic panel, lipid panel, vitamin D, ferritin, and HbA1c. For patients open to it, hormone panels evaluate where they sit in the perimenopause-to-menopause transition. The conversation is explicit about the interaction between hormonal status and weight loss strategy.
Treatment planning then accounts for the full picture. Some patients are best served by GLP-1 treatment alone, with the hormonal symptoms managed separately or not at all. Some are best served by hormone therapy first, with weight management revisited after hormonal status is stable. Some benefit from both approaches launched in coordination, with each treatment adjusted as the patient responds. The goal is a single coherent plan, not two unrelated services.
Resistance training guidance, protein targets, and bone health protocols are built into the plan from the start. Follow-up visits track multiple markers, not just the scale, because the cardiovascular and metabolic improvements often outpace the weight loss in clinical importance for this population. Schedule a free consultation to talk through how a combined plan would look for your specific situation.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
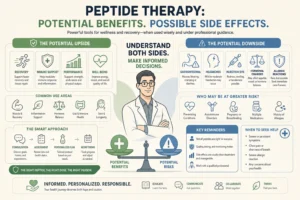
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never