Skin Tightening After Weight Loss: Non-Surgical Options Compared
Loose skin after weight loss has more non-surgical options than ever. Here is how the main skin tightening approaches compare and how to choose one.
If you are taking semaglutide, tirzepatide, or another GLP-1 medication, you have probably seen the headlines about muscle loss. Social media is filled with warnings about shrinking muscles and weakened strength. The concern is valid, but it is often misunderstood. Much of what gets reported as “muscle loss” is not actually skeletal muscle at all.
The clinical data tells a more nuanced story: GLP-1 medications do not uniquely destroy muscle. The body composition changes they produce are similar to what happens with any significant weight loss. And with the right combination of nutrition, exercise, and supportive therapies, patients can preserve lean mass while still benefiting from the powerful fat-reducing effects of these medications.
GLP-1 medications like semaglutide cause significant weight loss, but up to 39% of that loss can come from lean mass rather than fat. However, much of the reported “lean mass” loss is actually from the liver and body water, not skeletal muscle. Combining adequate protein intake (1.2 to 1.6 g/kg daily), consistent resistance training, and targeted therapies like peptide therapy can protect your muscle while maximizing fat loss.

GLP-1 receptor agonists cause lean mass loss because any significant calorie deficit triggers the body to break down both fat and lean tissue for energy. Semaglutide and tirzepatide suppress appetite and slow gastric emptying, often reducing daily calorie intake by 20 to 35%. When calorie intake drops that sharply, the body does not exclusively burn stored fat. It also catabolizes protein from lean tissue, especially when protein intake is insufficient or physical activity declines.
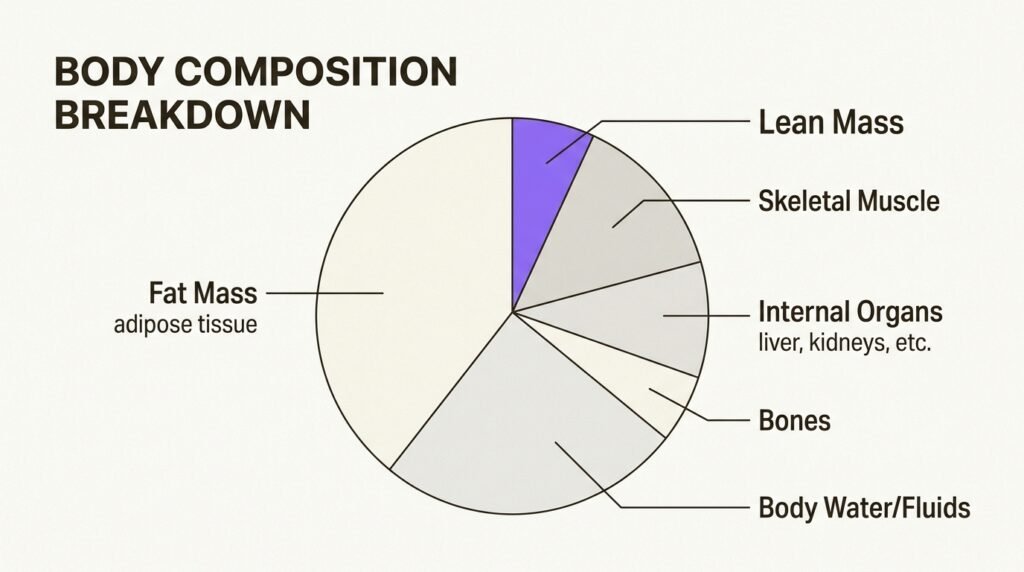
But the critical distinction is what “lean mass” actually means. When researchers report that 40% of weight lost came from “lean mass,” they are not talking exclusively about skeletal muscle. Lean mass includes internal organs (particularly the liver, which shrinks as fatty liver disease improves), body water, connective tissues, and water trapped in fat tissue. A comprehensive review in Pharmacological Research confirms that skeletal muscle changes with GLP-1 treatment appear to be “adaptive,” aligning with what you would expect given the amount of weight lost (Pereira et al., 2025).
An exercise physiologist at UC Davis Health clarified this point directly: “We are losing around 20% of muscle mass, but that is not different from diets that restrict calorie intake. Much of the reported 40% lean mass loss with GLP-1 use is coming from the liver.” The actual skeletal muscle impact is far less dramatic than the headlines suggest.
The landmark STEP 1 trial provides the most detailed body composition data for semaglutide. DXA analysis of a 140-participant subgroup showed that total lean body mass decreased by 9.7% over 68 weeks, while fat mass decreased by 19.3%. Lean tissue accounted for approximately 39% of total weight lost (Wilding et al., NEJM, 2021). That percentage sounds alarming in isolation, but context matters.
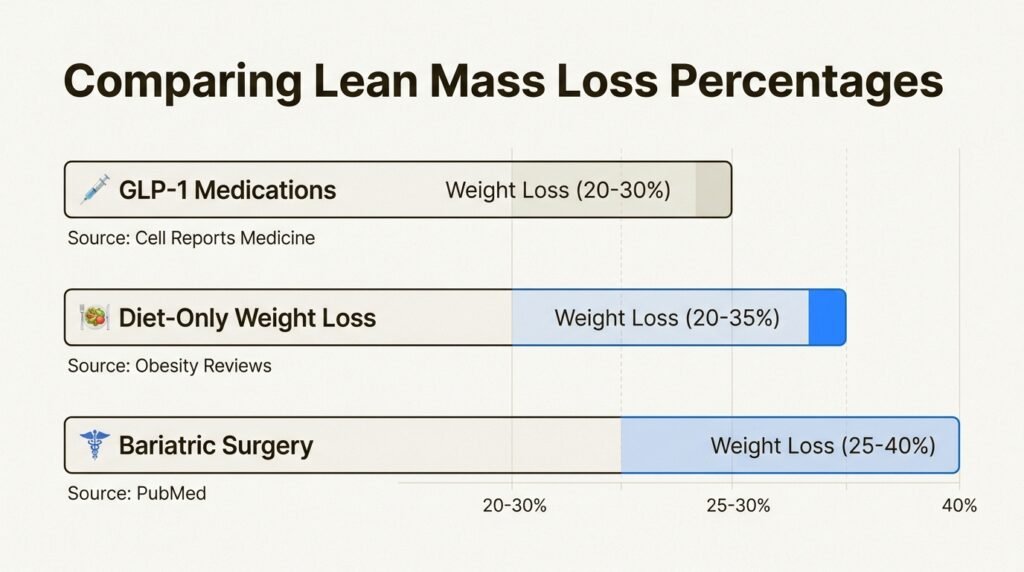
A 2022 systematic review in Obesity Reviews found that GLP-1 associated weight loss showed comparable or slightly better muscle preservation than diet-only approaches. When people lose weight through calorie restriction alone, they typically lose 20 to 35% from lean tissue. GLP-1 medications perform similarly or sometimes better. Research published in Cell Reports Medicine in 2026 concluded directly: weight loss with GLP-1 medicines does not result in a disproportionate loss of muscle mass or function.
Importantly, even though total lean mass decreased, the proportion of lean mass relative to total body weight actually increased in semaglutide patients. That means overall body composition improved: patients had a higher percentage of lean tissue and a lower percentage of fat after treatment. Improved insulin sensitivity and reduced muscle fat infiltration also led to better muscle quality, even when total volume decreased slightly.
Patients on GLP-1 medications should consume 1.2 to 1.6 grams of protein per kilogram of body weight daily to meaningfully preserve lean mass. For a 200-pound patient, that translates to roughly 110 to 145 grams of protein each day, considerably more than the standard dietary recommendation of 0.8 g/kg. A randomized trial by Longland et al. demonstrated that participants consuming higher protein during an energy deficit gained lean body mass while losing fat mass, compared to a lower-protein group that lost lean tissue (American Journal of Clinical Nutrition, 2016).
This is where GLP-1 patients face a unique challenge. The same appetite suppression that drives weight loss also makes it difficult to eat enough protein. Body Works addresses this by recommending protein-dense food choices at every meal (Greek yogurt, lean poultry, fish, eggs, legumes), strategic use of protein supplementation between meals, and timing protein intake around workouts for maximum muscle protein synthesis. Spreading protein across four to five smaller meals rather than two or three large ones improves absorption.
For patients following best practices for medical weight loss injections, prioritizing protein from the first week of treatment prevents the deficit that accelerates lean mass breakdown later.
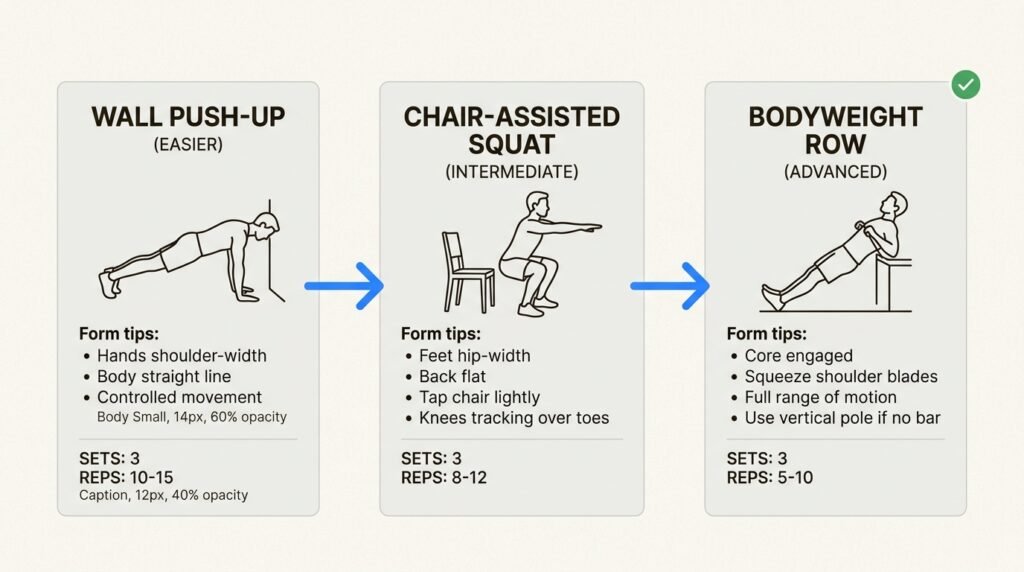
Resistance training is the single most effective intervention for preserving lean mass during GLP-1 treatment. Lifting weights or performing bodyweight exercises sends a direct signal to muscles that they are needed, overriding the catabolic signals created by calorie restriction. Two to three sessions per week focusing on compound movements (squats, presses, rows) is sufficient. Starting from scratch? Begin with wall push-ups, chair-assisted squats, and supported bridges, then progress as strength improves. Consistency matters more than intensity.
Beyond exercise, peptide therapy offers a targeted approach to protecting lean mass that works synergistically with GLP-1 medications. Peptides such as CJC-1295 and ipamorelin stimulate natural growth hormone secretion, which plays a critical role in muscle maintenance and fat metabolism. For patients on semaglutide who are concerned about losing strength, adding peptide therapy creates a dual approach: GLP-1 medications drive appetite control and fat reduction, while peptides support the anabolic environment muscles need to stay intact.
For patients with clinically low testosterone, hormone optimization through TRT can further improve the ratio of fat lost to muscle preserved. Low testosterone is common in patients with obesity and directly impairs the body’s ability to maintain muscle mass during caloric restriction. Heymsfield et al. demonstrated that pharmacological approaches targeting anabolic pathways can shift body composition toward fat loss while preserving or gaining muscle in adults with obesity (JAMA Network Open, 2021).
| Strategy | Effectiveness for Muscle Preservation | Best For |
|---|---|---|
| High Protein Intake (1.2-1.6 g/kg/day) | High; reduces lean mass loss by up to 50% | All GLP-1 patients |
| Resistance Training (2-3x/week) | Very High; strongest single intervention | All patients able to exercise |
| Peptide Therapy (GH-releasing peptides) | High; supports anabolic signaling | Patients with significant muscle concerns |
| Testosterone Replacement Therapy | High; restores hormonal muscle support | Patients with clinically low testosterone |
| No Intervention (GLP-1 only) | Low; 25-40% of weight lost is lean mass | Not recommended |
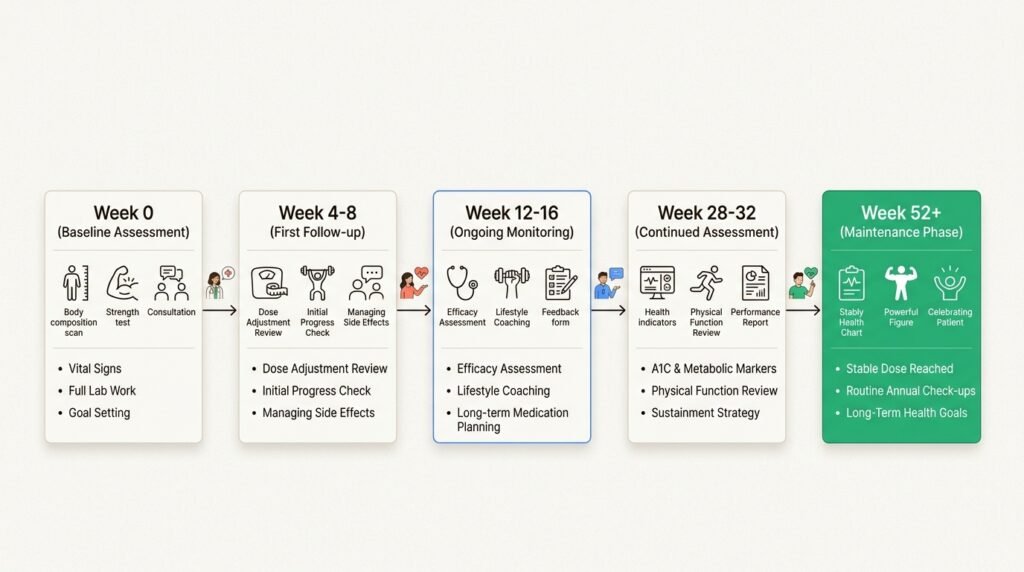
Patients who combine medication with diet and exercise consistently achieve better body composition outcomes than those who rely on medication alone. At Body Works, every medical weight loss program includes baseline body composition assessment, protein optimization guidance, follow-up monitoring at 4 to 8 weeks, and ongoing assessments every 12 to 16 weeks during active treatment. Your provider tracks not just the scale but waist circumference, strength markers, and metabolic indicators to ensure you are losing fat, not the muscle that keeps you strong.
Body Works in Franklin and Nolensville, TN offers GLP-1 therapy, peptide therapy, and hormone optimization under one roof, giving patients access to every evidence-based tool for protecting lean mass during weight loss. Dr. Donald Vollmer evaluates your body composition, hormone levels, and health history to build a plan tailored to your specific risk profile. Schedule a Free Consultation to discuss how to protect your muscle while achieving your weight loss goals.
Clinical trials show approximately 25 to 39% of weight lost on semaglutide comes from lean body mass, but much of that is liver volume reduction and body water, not skeletal muscle. The actual skeletal muscle loss is comparable to what occurs with any form of calorie restriction. With proper protein intake and resistance training, patients can significantly reduce lean mass loss.
Yes. A combination of resistance training at least two to three times per week and protein intake of 1.2 to 1.6 g/kg per day has been shown to preserve and even increase lean mass during caloric restriction. Adding peptide therapy or testosterone optimization can further support muscle growth in appropriate candidates.
The recommended intake is 1.2 to 1.6 grams of protein per kilogram of body weight daily. For most patients, this means 100 to 150 grams of protein per day. Spreading intake across four to five meals and prioritizing protein-dense sources like eggs, poultry, fish, and whey protein optimizes muscle protein synthesis.
Costs vary based on the combination of therapies in your plan. GLP-1 medication, protein guidance, and exercise programming are included in the standard weight loss program. Peptide therapy and hormone optimization are additional services with separate pricing discussed during your consultation.
Yes. Both the Franklin and Nolensville, TN locations include baseline body composition assessment and ongoing monitoring as part of every weight loss program. Your provider tracks lean mass, fat mass, and functional markers to ensure your treatment is producing the right kind of weight loss.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
Loose skin after weight loss has more non-surgical options than ever. Here is how the main skin tightening approaches compare and how to choose one.
Rapid weight loss can leave the face looking hollow. Here is an honest look at what dermal fillers, biostimulators, and collagen support can and cannot
GLP-1 microdosing and maintenance dosing are physician-guided strategies, not internet shortcuts. Learn what each term means, why interest is growing, what the evidence shows, and
Once a GLP-1 medication quiets your appetite, knowing what to eat matters more than ever. This practical guide covers protein targets, the foods that worsen
Tirzepatide is available now for physician-supervised weight loss in Franklin and Nolensville, TN. Here is what the medication is, how local availability differs from telehealth

Retatrutide’s phase 2 trial produced an average of about 24% body weight loss, higher than the numbers seen with approved medications like tirzepatide and semaglutide.