Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
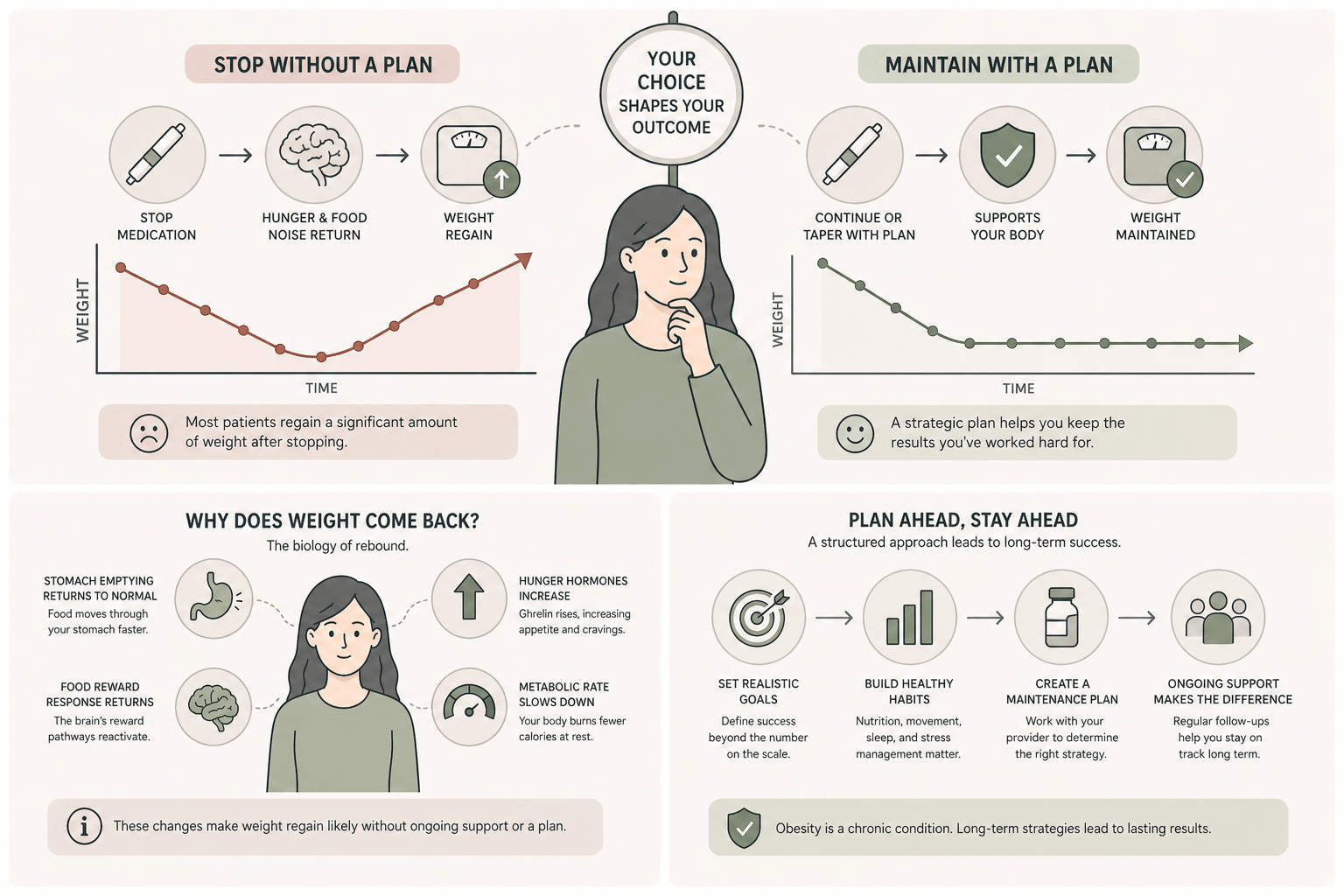
Most patients on semaglutide therapy or tirzepatide eventually ask the same two questions: how long do I need to take this, and what happens if I stop? Those questions feel different, but they are really the same conversation viewed from two angles. The answer matters because the choices you make about discontinuing or maintaining your medication shape whether your hard-won progress lasts or disappears.
Here is what the clinical research shows. Stopping a GLP-1 medication abruptly, without any maintenance plan, leads to substantial weight regain in most patients. This is not a willpower problem. It is biology. The same hormones the medication suppresses come back online when the medication leaves your system, and your appetite and fullness signals reset to where they started.
That is not the end of the story. Patients who plan their transition carefully, often with a tapered dose or a structured maintenance phase, can preserve a meaningful share of their weight loss long term. The strategy starts long before you reach your goal weight. It is built into a physician-supervised program from the beginning, and it is the difference between viewing medical weight loss as a sprint and viewing it as a long-term health intervention.
The most rigorous data on semaglutide discontinuation comes from a follow-up to the STEP 1 trial. Patients who lost an average of 17.3% of their body weight over 68 weeks on semaglutide 2.4 mg were taken off the medication and followed for one additional year. By week 120, they had regained roughly two-thirds of the weight they originally lost (Wilding et al., Diabetes, Obesity and Metabolism, 2022).
This regain pattern was not caused by patients abandoning their lifestyle changes. The trial included continued behavioral counseling. The weight came back primarily because the medication was no longer suppressing appetite, slowing gastric emptying, or amplifying satiety signals. When the drug effect ended, the underlying biology of obesity returned.
The takeaway is not that semaglutide does not work. It plainly does. The takeaway is that the medication treats a chronic condition, and most patients need a long-term strategy that does not assume a clean exit at the end of an active loss phase.
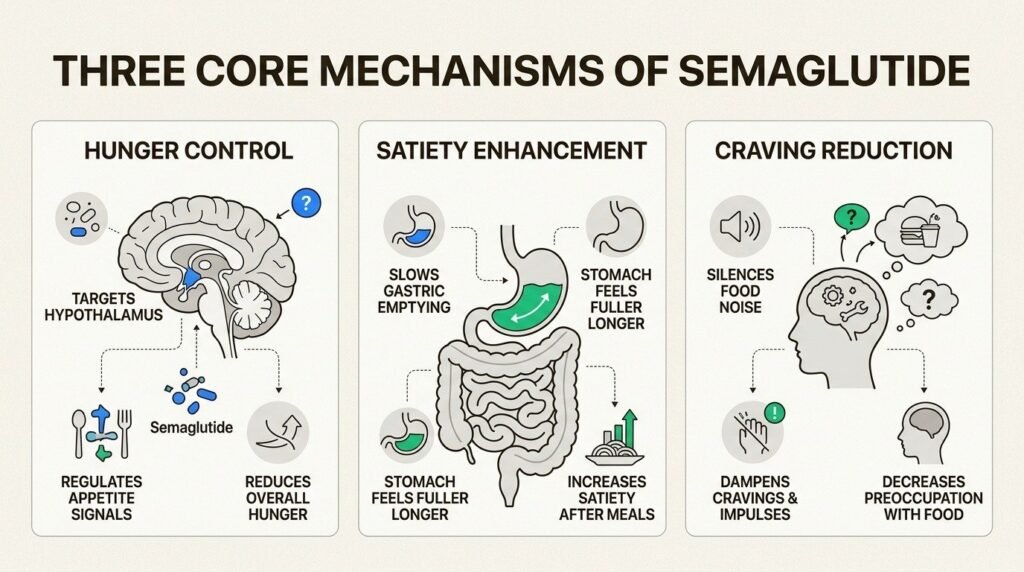
GLP-1 medications work through several mechanisms simultaneously. They activate GLP-1 receptors in the brain and gut, reducing hunger signals and increasing the sense of fullness after meals. They slow the rate at which food leaves the stomach, which extends satiety. They also improve insulin sensitivity and dampen the reward response to high-calorie food.
When the medication is discontinued, all four of those effects reverse on a similar timeline. Ghrelin, the hormone that drives appetite, climbs back to baseline within weeks. Gastric emptying returns to normal speed. The food-reward circuits in the brain stop being suppressed. Patients describe this as the return of food noise, an experience that becomes especially noticeable after months of relative quiet on medication.
Body weight regulation is also defended by what researchers call metabolic adaptation. After significant weight loss, the body lowers its resting metabolic rate and increases hunger signaling in an attempt to restore lost mass. This effect is documented across all weight loss interventions and is one of the reasons sustained loss is harder than initial loss (National Institute of Diabetes and Digestive and Kidney Diseases).
Tirzepatide produces larger initial weight loss than semaglutide in head-to-head clinical comparisons, but the discontinuation pattern is very similar. The SURMOUNT-4 trial randomized patients who had lost weight on tirzepatide to either continue the medication or switch to placebo. The continued group preserved their weight loss. The placebo group regained about 14% of body weight over the next year, while the continuation group lost an additional 5.5% (Aronne et al., JAMA, 2024).
The pattern is consistent across both medications: continued treatment preserves weight loss, abrupt discontinuation reverses much of it. Tirzepatide may produce a slightly slower regain trajectory than semaglutide because of its dual GIP and GLP-1 mechanism, but both drugs require a thoughtful exit plan.
For patients weighing the choice between the two medications, the regain risk is similar enough that it should not drive the decision. Choosing between semaglutide and tirzepatide turns on tolerance, response, and your provider’s clinical judgment, not on which one is easier to stop.
Major medical organizations now classify obesity as a chronic disease that often requires long-term treatment, similar in framing to hypertension or type 2 diabetes. The American Medical Association formally adopted this classification in 2013, and the American Heart Association reaffirmed it in 2021. From this perspective, expecting a fixed treatment duration for obesity is like expecting a fixed treatment duration for high blood pressure. Some patients can taper or discontinue successfully. Many cannot, and that is a clinical reality, not a failure of effort.
In practice, patients fall into a few patterns. Some stay on a maintenance dose indefinitely. Some taper to a lower dose and stay there. Some complete an active loss phase, transition off the medication entirely, and rely on intensified lifestyle support to hold their weight. The right path depends on your starting weight, your goal weight, your metabolic profile, your response during the active phase, and your tolerance for the medication.
What rarely works is choosing a duration in advance based on a target weight alone. Patients who set themselves a hard stop at month 6 or month 12 and then discontinue without a maintenance plan see the regain pattern described above. Setting the duration question aside until later in treatment, and revisiting it with your provider as data accumulates, leads to better outcomes.
Tapering means gradually reducing the dose over weeks or months, often to a lower maintenance dose, rather than stopping at the therapeutic dose abruptly. Cold-turkey discontinuation is the pattern that produces the regain numbers from STEP 1 and SURMOUNT-4.
A typical tapering protocol might step a patient down from 2.4 mg semaglutide to 1.7 mg, then 1 mg, then 0.5 mg over three to six months, observing weight stability at each step. Some patients hold at 0.5 mg as a long-term maintenance dose. Others continue down and eventually discontinue, with the lifestyle scaffolding strong enough to hold the weight.
The clinical judgment about when and how to taper involves more than the scale. Body composition, lab work, hunger and satiety self-reports, and lifestyle adherence all factor in. This is where physician supervision earns its keep. A retail subscription model that ships the same dose every month does not have the structure to support a thoughtful taper.
At Body Works, the maintenance question is part of the conversation from your first consultation, not something raised at the end. The active loss phase, typically four to six months, sets the framework for what comes next. Lab work establishes a baseline and tracks metabolic markers. Body composition measurements separate fat loss from muscle loss, which matters because preserving muscle on GLP-1 medications is one of the strongest predictors of weight stability after the active phase.
As patients approach a target weight, the plan transitions. Visits often shift from monthly to every six to eight weeks. Doses are reviewed and adjusted. Nutritional guidance moves from caloric deficit to maintenance, and resistance training becomes more central. For some patients, the maintenance phase is permanent. For others, it is a stepping stone toward eventual discontinuation. Either path is legitimate, and the path that fits you is the one your data and your provider agree on.
The decision points and red flags worth tracking are listed in our guide to what to ask before signing up for medical weight loss. If a clinic does not discuss what happens after you reach your goal during the initial consultation, that is itself a signal about how the program is built.
There is no single test that says you are ready to taper. A combination of factors usually points in the right direction. Stable weight for at least three months at the maintenance dose. Lab markers that have moved into healthy ranges and stayed there. Established habits around protein intake, resistance training, sleep, and stress management. A realistic understanding that taper attempts sometimes fail and that returning to a maintenance dose is not a setback.
Patients who try to taper without those foundations typically regain. Patients who try to taper with those foundations sometimes still regain, and that is also useful information. A failed taper attempt is not a failure of the patient. It is data that says the body is still defending a higher set point and that ongoing medication is likely the right long-term strategy for that individual.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never