Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never get told that. This is the gap that peptides for women are meant to address.
The first system is ovarian. Estrogen and progesterone fluctuate, then drop, between the late 30s and mid 50s. The second is almost never discussed: your pituitary’s nightly pulses of growth hormone fall by roughly half between your 20s and your 50s, with the steepest drop alongside the loss of deep sleep. Van Cauter and colleagues, JAMA, 2000, documented that slow wave sleep falls from about 18.9 percent of the night in early adulthood to roughly 3.4 percent by midlife, with growth hormone secretion declining in lockstep.
This is where peptides deserve a careful look. They are not a replacement for hormone therapy and not a workaround for sleep, food, and strength training. They are a signaling tool that may help the pituitary side recover some of what time has dialed back. At Body Works in Franklin, TN and Nolensville, TN, peptide therapy is one piece of an integrated plan that also weighs hormones, labs, and lifestyle.
Midlife metabolic change is not one event but two overlapping declines. Perimenopause shifts the sex hormone signaling, while the somatotropic axis (growth hormone and IGF-1) fades on its own clock.
Ovarian estrogen begins to swing widely in the early 40s, and that fluctuation, more than the eventual drop, drives most early symptoms. A clinical overview of perimenopause from Mayo Clinic notes that women typically enter perimenopause in their mid 40s, often four to eight years before their final period, with hot flashes, sleep disruption, mood shifts, and changes in body composition. The ACOG Menopause Years FAQ ties the same vasomotor and sleep symptoms to fluctuating ovarian output.
Running in parallel is the somatopause. Pituitary growth hormone release falls in a predictable, age-linked pattern independent of menstrual status. Because growth hormone supports lean tissue, fat oxidation, and overnight repair, its decline shows up as fatigue, slower recovery, and stubborn central fat. Peptide therapy targets this second axis.
Peptides are short chains of amino acids that act as biological messengers, telling tissues when to release a hormone, repair a tendon, or dampen inflammation. The ones relevant to women in their 40s and 50s are mostly growth hormone secretagogues, which prompt the pituitary to release its own growth hormone in a pulse that mimics what the body did at 25.
For background, see the pillar overview of how peptide therapy works and the plain-English explainer on what peptides actually are.
Growth hormone secretagogues like sermorelin, CJC-1295, and ipamorelin do not flood the body with synthetic hormone; they restore a signal. That distinction matters, because the pulsatile pattern preserves the negative feedback loop that guards against the side effects of direct growth hormone injections. Teichman and colleagues, in the Journal of Clinical Endocrinology and Metabolism, 2006, showed that CJC-1295 raised mean growth hormone and IGF-1 in healthy adults for several days after a single dose.
For midlife fatigue and broken sleep, the relevant tools are growth hormone releasing peptides. The pituitary’s largest growth hormone pulse of the day happens in the first cycle of slow wave sleep. When that pulse weakens, women wake unrefreshed and feel wired but tired in the evening.
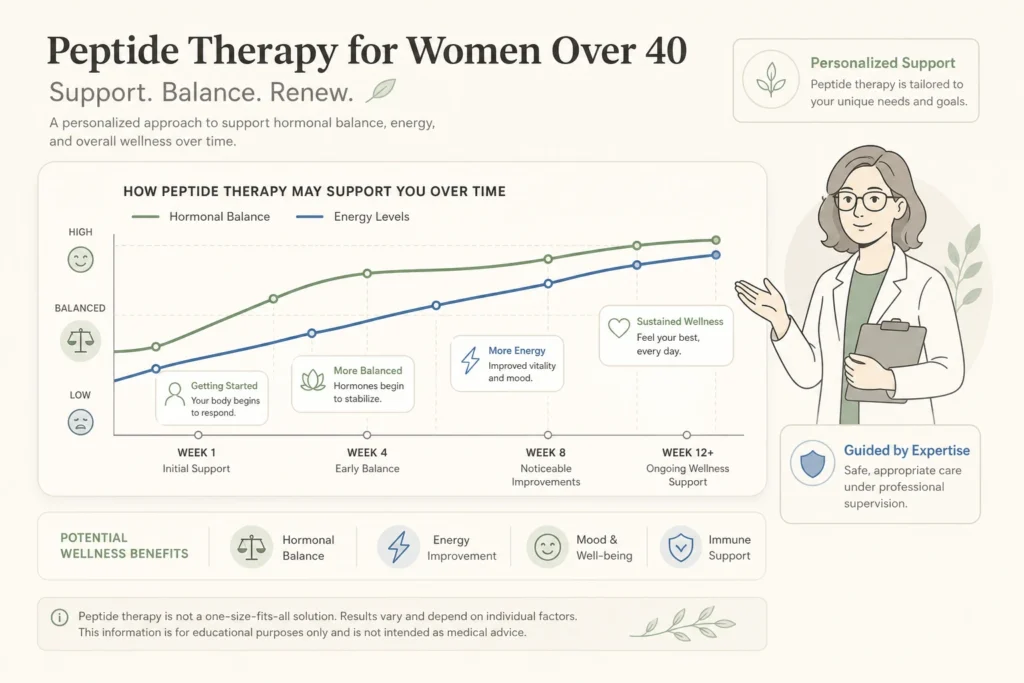
Sermorelin and the CJC-1295 plus ipamorelin combination both push the pituitary toward a younger release pattern, increasing slow wave sleep and overnight growth hormone exposure. In practice, most women describe deeper sleep within two to four weeks, followed by daytime energy that holds through the afternoon rather than collapsing at 3 p.m. The peptide is not a stimulant; it restores the overnight repair window.
Yes, but with realistic framing: peptide therapy supports the work, it does not replace protein, resistance training, and sleep.
The reason body composition shifts after 40 is mechanical. Lean mass falls about 3 to 5 percent per decade from the 30s onward unless strength training defends it, and the metabolic engine shrinks with it. The National Institute on Aging guidance on strength training and aging treats resistance exercise as the first-line intervention because it directly counters age-related muscle loss and the resulting drop in basal metabolic rate.
Where peptides earn their place is recovery and visceral fat. Growth hormone supports lipolysis (fat release from storage) and protein synthesis (muscle repair). The clearest evidence comes from tesamorelin, a growth hormone releasing hormone analog studied in a different population, where Stanley and colleagues in Clinical Infectious Diseases, 2012 documented reductions in visceral adipose tissue and improved lipid profiles. Sermorelin and CJC-1295 engage the same axis. Pair the peptide with resistance training, adequate protein, and sleep, and the body responds; skip those inputs, and it has nothing to act on. When central fat is metabolic rather than growth hormone driven, a medical weight loss evaluation can clarify which lever matters most.
Peptide therapy is not a fit for every woman, and candidacy is the part most direct-to-consumer telehealth services skip. A safe protocol starts with bloodwork, a medication review, and an honest medical history.
The clearest contraindications for growth hormone secretagogues are active malignancy, untreated diabetic retinopathy, severe untreated sleep apnea, and pregnancy. A personal history of hormone-sensitive cancer calls for a more conservative conversation, since the IGF-1 axis is active in those tissues. Common, manageable side effects include injection site redness, mild first-week water retention, and occasionally brief tingling that fades as the dose stabilizes.
Hormone therapy and peptide therapy are not the same intervention, and one does not replace the other. The Endocrine Society menopause treatment overview remains the standard patient reference for hormone therapy decisions. Hormone replacement targets the ovarian axis directly; peptides target a different signal. The two can coexist and are best evaluated together rather than as either-or.
The most useful framing is that peptides for women address what hormone replacement does not. Estrogen, progesterone, and testosterone replacement help with vasomotor symptoms, bone density, and mood, but they do not restore the growth hormone pulse during sleep or rebuild the recovery window the somatopause takes away.
An integrated plan starts with labs, a symptom inventory, and a candidacy review for both axes. If hormone therapy is indicated, that conversation happens in the same evaluation, so both sides are weighed together. If peptide therapy is appropriate, the protocol is matched to the goal, usually CJC-1295 with ipamorelin for sleep and recovery, or sermorelin as a softer starter. Patients in Franklin and Nolensville begin with a free consultation, not a protocol on day one.
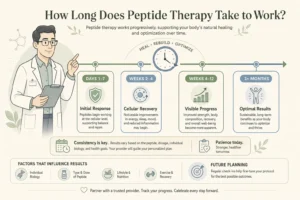
| Timeframe | What Most Women Notice | What Drives It |
|---|---|---|
| Weeks 1 to 2 | Slight injection site redness; sleep starts to deepen for some | Restored evening growth hormone pulse |
| Weeks 3 to 6 | Consistent deeper sleep, steadier daytime energy, faster recovery from workouts | Cumulative effect of nightly slow wave sleep restoration |
| Months 2 to 4 | Visible body composition shift when paired with resistance training and protein | Improved lean mass retention and fat oxidation during recovery |
| Months 4 to 6 | Skin and hair texture changes for some women; sustained energy | Downstream IGF-1 effects on collagen turnover |
The first thing to disappear is fatigue. Body composition follows, and it follows the work, not the medication. Women who treat peptides as a license to skip strength training or sleep do not see the result; women who treat the peptide as the missing signal underneath a real plan generally do. If the protocol stops, the gained signal fades and most women drift back toward baseline over the following months.
If the version of yourself you remember at 35 feels far away, the next step is not to order a peptide online. It is to find out which signaling system is fading and what a safe, monitored protocol would look like for your labs and history. Body Works evaluates hormones and peptides together, in the same conversation.
Both offices offer free consultations. Walking through your labs, history, sleep, and goals with a provider takes about an hour and commits you to nothing. You leave knowing whether peptide therapy is a reasonable fit, whether hormone therapy belongs in the plan, and what a realistic six month picture looks like. To prepare, the what to expect at a first peptide therapy appointment walkthrough covers the visit step by step.
Ready to find out whether peptide therapy is right for you? Schedule a Free Consultation at the Franklin or Nolensville office. Call Franklin at (615) 790-2548 or Nolensville at (615) 941-1000 with questions before you book.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
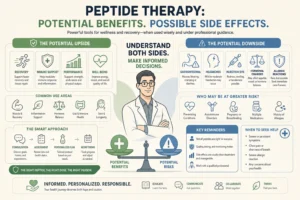
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin
“Weeks to months.” That is the answer almost every peptide therapy provider hands a patient who asks how long it takes to feel something. It