GLP-1 Microdosing and Maintenance Dosing Explained
GLP-1 microdosing and maintenance dosing are physician-guided strategies, not internet shortcuts. Learn what each term means, why interest is growing, what the evidence shows, and
This guide walks through what the research on BPC-157 tissue repair actually shows, where the strongest evidence sits, what the FDA 503A compounding framework allows in 2026, and how a physician-supervised program at Body Works in Franklin, TN and Nolensville, TN evaluates candidacy. The goal is an honest picture of the mechanism, the benefits, and the limits before you spend a dollar on any peptide protocol.
BPC-157 is a synthetic chain of 15 amino acids modeled on a sequence found in human gastric juice. The name stands for Body Protection Compound, which captures the original research interest: a small molecule the gut produces that appears to support tissue repair across multiple organ systems. Researchers synthesized BPC-157 in the lab to study that sequence in isolation, and the bulk of the published work since the 1990s has examined how it behaves in animal models of injury.
A recent systematic review by McGuire et al., emerging use of BPC-157 in orthopaedic sports medicine, HSS Journal, 2025 summarizes the field this way: animal evidence for accelerated soft-tissue healing is broad and reproducible, but only three small human pilot studies exist, covering intraarticular knee pain, interstitial cystitis, and intravenous safety and pharmacokinetics. That is the honest framing every reader should start with. The mechanism story is rich. The human outcome story is still being written.
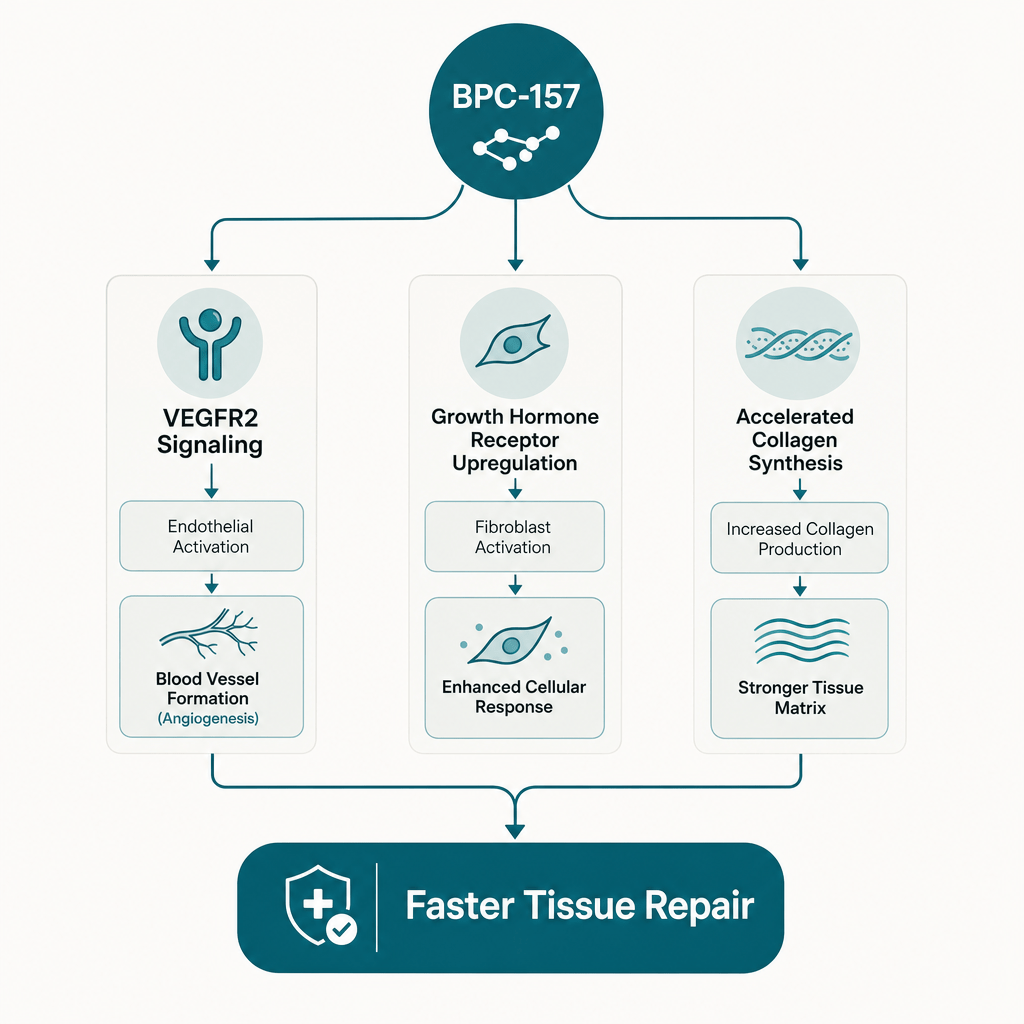
The strongest preclinical signal for BPC-157 sits in tendon and ligament repair. In animal models of Achilles transection, medial collateral ligament tears, and rotator-cuff injury, the peptide has consistently accelerated functional recovery and improved tissue organization on histology. The proposed mechanism involves several pathways at once. The peptide triggers VEGF receptor signaling that stimulates new blood vessel growth into the wound bed, amplifies growth hormone receptor sensitivity in fibroblasts so existing repair signals carry further, and accelerates collagen organization in tendon tissue.
A narrative review by McGuire et al., regeneration or risk, Current Reviews in Musculoskeletal Medicine, 2025 concludes that BPC-157 demonstrates reproducible regenerative and cytoprotective effects in preclinical work, with effects on tendon cell outgrowth, fibroblast survival under stress, and migration into damaged tissue. Earlier mechanistic work by Chang et al., tendon outgrowth and cell migration, Journal of Applied Physiology, 2011 linked those effects to FAK-paxillin signaling, a pathway tendon fibroblasts use to crawl into a healing wound. The pattern is consistent across labs. The question is how reliably those animal findings translate to humans.
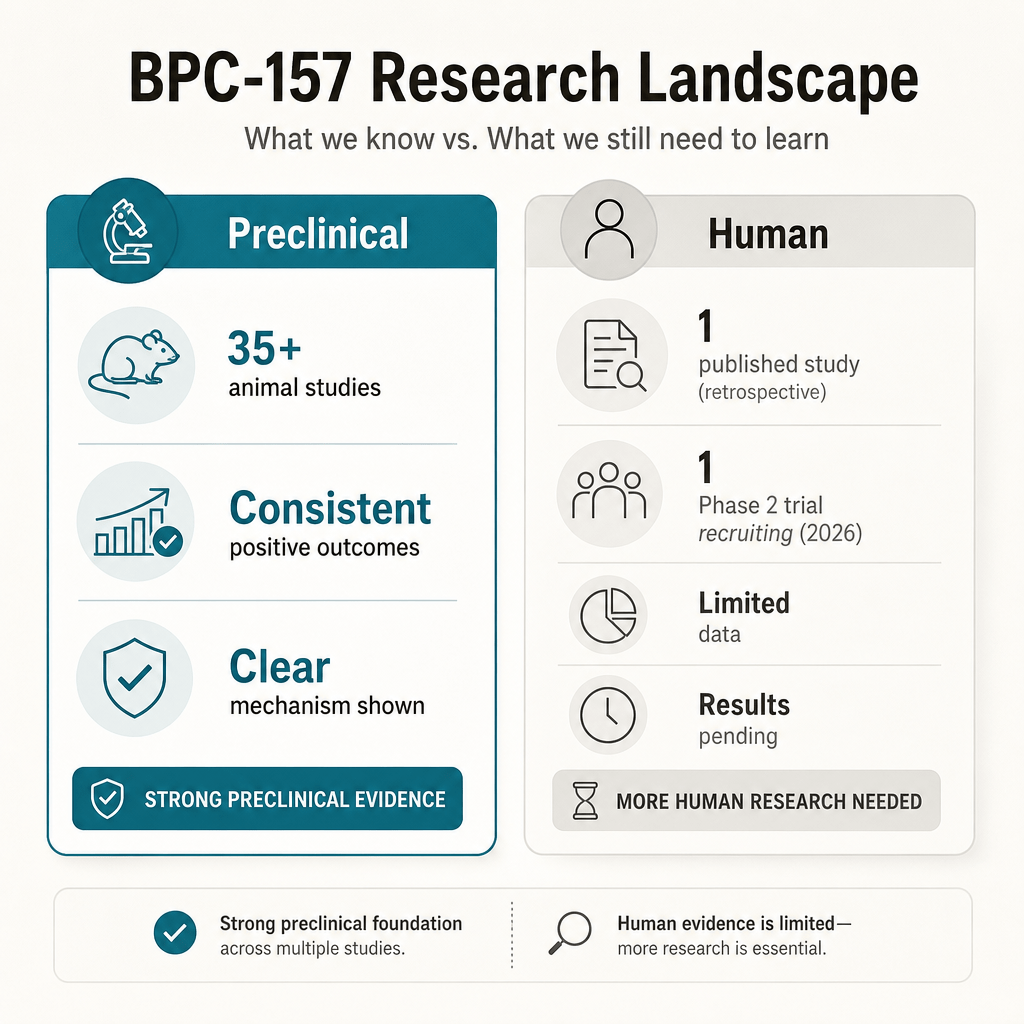
The evidence splits sharply into two buckets. Preclinical work is broad and consistent. Human work is sparse and early. A 2025 systematic review screened 544 articles and included 36 studies, of which 35 were preclinical animal studies and only one was a human trial. That ratio is the most important fact a patient can know before starting a protocol.
On the animal side, the signal is reproducible across labs. Rats with transected Achilles tendons healed with greater tensile strength and faster functional recovery on systemic BPC-157 dosing. Rats with medial collateral ligament injuries showed faster biomechanical recovery on both local and systemic administration. Rabbit bone-defect models showed acceleration comparable to autologous grafts, with the strongest effect at bone-to-tendon junctions. On the human side, one retrospective case series of 17 patients receiving intraarticular knee injections reported sustained pain relief over six to twelve months, but there was no control group, no blinding, and no randomization. A Phase 2 randomized controlled trial of BPC-157 for acute hamstring strain is now recruiting, with results expected in early 2027. That trial will be the first rigorous human efficacy test of this peptide.
BPC-157 was originally isolated for its gut-protective effects, and that line of research is older and broader than the orthopedic work. In rodent models of inflammatory bowel disease, esophageal injury, gastric ulcer, and toxin-induced colitis, the peptide has accelerated mucosal healing and reduced inflammatory markers. The proposed mechanism overlaps with the tendon story: improved local blood flow, stabilized nitric oxide signaling, and protection of epithelial cells against oxidative stress.
A 2018 review by Sikiric et al., BPC 157 and angiogenic growth factors, Current Pharmaceutical Design, 2018 traces the angiogenesis hypothesis across both gastrointestinal and musculoskeletal injury models, arguing the peptide acts as a general protector of damaged vascular networks. Clinically, the most honest takeaway is that BPC-157 has plausible biology for gut healing, animal data that is genuinely interesting, and no large human trials confirming the effect. Patients with active gastrointestinal disease should be managed by a gastroenterologist using established therapies, not by self-administered peptides ordered online.
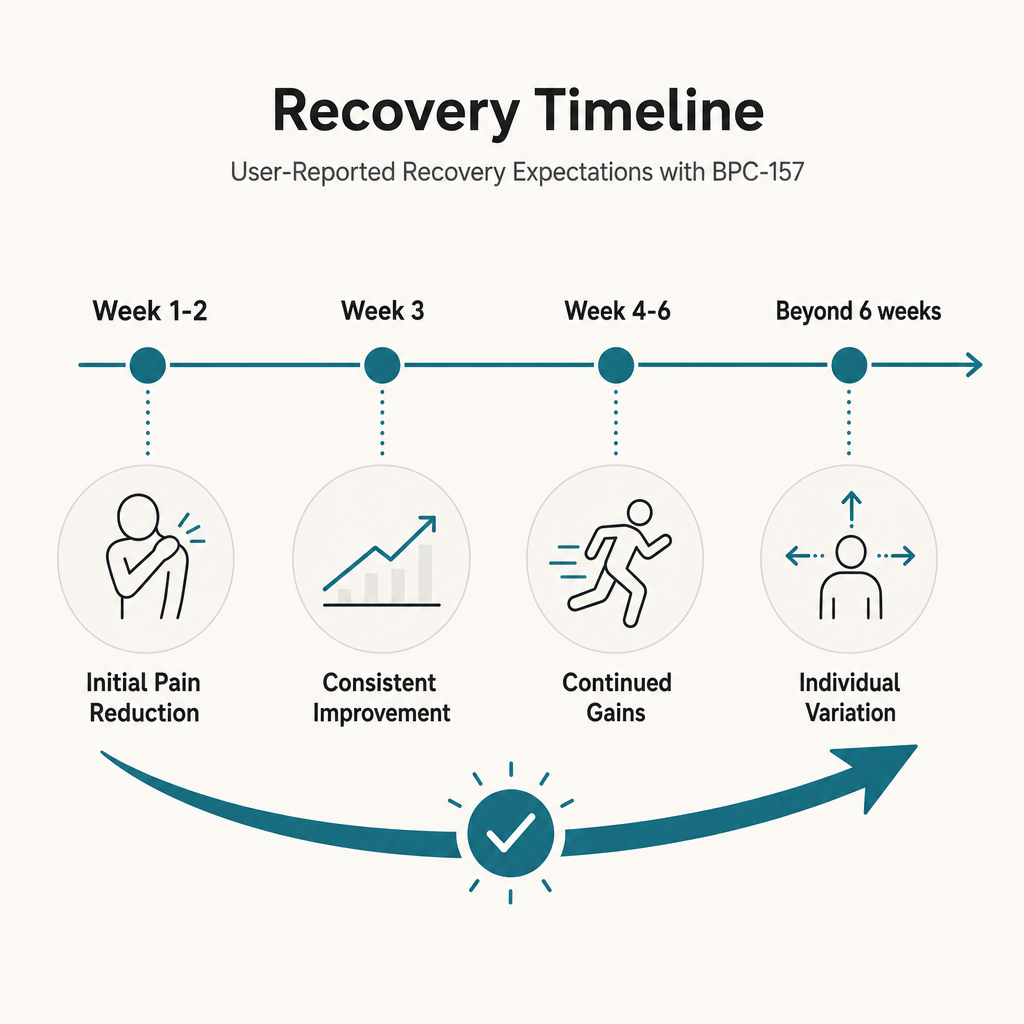
Published animal data and clinical experience inside supervised peptide programs converge on a few honest expectations. The early subjective signal, usually a reduction in pain or stiffness, often appears in the first two to three weeks of a protocol. Functional improvement in joint mobility, range of motion, or load tolerance commonly appears between weeks three and six. Structural change continues underneath those signals for longer than the patient feels it, which is why protocols are usually run for at least eight to twelve weeks rather than stopped at first relief.
Several variables move the timeline. Acute injuries with intact blood supply respond faster than chronic, degenerative tissue. Patients who pair the peptide with structured physical therapy, adequate protein intake, and seven to eight hours of sleep do measurably better than patients who treat BPC-157 as a standalone fix. Patients with active inflammatory conditions, uncontrolled blood sugar, or significant nicotine exposure tend to respond more slowly. Honest peptide programs are measured in months, not days, and the patients who do best understand that.
Safety data for BPC-157 has looked favorable in the published literature, which is one reason the peptide became popular before the regulatory picture caught up. Animal studies have not identified a clear toxic threshold, and the small human pilot studies have not surfaced major adverse events. That is meaningfully different from proven safe. Long-term outcomes and effects in patients with comorbid disease are still missing.
The honest caveats matter for anyone considering treatment. BPC-157 has not been studied in pregnant or breastfeeding patients and should be avoided in those groups. Patients with a history of cancer face a theoretical risk because the peptide promotes angiogenesis, which is also the process that supports tumor growth, and there is not enough oncology safety data to use it confidently in that context. Patients with active autoimmune disease, uncontrolled diabetes, or significant kidney or liver dysfunction need individualized evaluation. Endocrine Society clinical practice guidance on hormone and peptide therapeutics consistently emphasizes that emerging compounds without large randomized trials require careful patient selection and active monitoring, not blanket use.
The compounding picture for BPC-157 changed in April 2026. On April 22, 2026, the FDA removed twelve peptides, including BPC-157, from Category 2 of the 503A bulk drug substances framework. Category 2 was the agency’s significant-safety-concerns list, and removal does not mean approval. It means the substance is no longer under that active concern designation while the formal review process continues. The Pharmacy Compounding Advisory Committee is scheduled to discuss BPC-157 and several other peptides at its July 2026 meeting to determine whether they belong on the formal 503A bulks list.
According to the FDA bulk drug substances under Section 503A page, only state-licensed pharmacists working under a physician prescription may compound bulk substances that meet the regulatory criteria, and the list is updated as new evidence arrives. For patients, the practical reading is that the compounding lane exists but is in active flux, and clinical use of BPC-157 belongs inside a physician relationship that watches the regulatory file closely. A deeper read of the April 2026 changes is available in the explainer on FDA peptide regulation in 2026, which sits alongside the broader complete guide to peptide therapy for context.
The patients most often considered for BPC-157 in physician-supervised peptide programs fall into a few clear groups. Active adults dealing with a slow-healing tendinopathy that has not responded fully to physical therapy, conservative orthopedic care, and time. Post-surgical patients trying to support soft-tissue recovery without compromising standard rehab. Patients recovering from a recent injury where the goal is to accelerate the early window of repair. Patients with a chronic gastrointestinal complaint that has been worked up by a specialist and remains symptomatic.
The patients who are not good candidates are equally important to name. Anyone with active malignancy or a recent history of it, given the angiogenesis question. Pregnant or breastfeeding patients. Patients seeking BPC-157 as a substitute for guided rehabilitation, which it is not. Patients with muscle loss after rapid weight reduction usually need a structured plan rather than a standalone peptide, and the medical weight loss program at Body Works is the right entry point for that group.
BPC-157 at Body Works sits inside a structured peptide protocol rather than as a one-off prescription. The first step is a consultation with the medical team to review goals, current medications, prior injuries, surgical history, and any oncology or autoimmune flags. Bloodwork is ordered when clinically indicated. If BPC-157 is appropriate, the protocol is built around the patient’s specific question: tendon recovery, post-surgical support, gut symptoms, or general regenerative goals. Sourcing comes from accredited 503A compounding pharmacies, and the team tracks the FDA regulatory file as it evolves.
This program-first framing matters because BPC-157 is a tool, not a treatment plan. The patients who do best understand the peptide is one input alongside physical therapy, sleep, nutrition, and patience. A useful companion read is the existing post on peptide authenticity and sourcing, which covers what to look for in a 503A compounder. New readers can also start with the plain-English guide to peptides if the broader category is still unfamiliar.
The right next step is a consultation, not a checkout. BPC-157 is not a supplement you buy off a shelf, and the patients who get the most out of it are the ones who treat it as a medical decision rather than a wellness purchase. A physician-supervised peptide therapy program at Body Works in Franklin and Nolensville includes the candidacy review, sourcing oversight, dosing structure, and the follow-up that the published literature and the current FDA framework both recommend.
If a slow-healing injury, post-surgical recovery, or persistent soft-tissue complaint has you researching peptides, the most useful thing you can do is talk to a physician who works with this category. Schedule a Free Consultation with the Body Works team. You can reach the Franklin office at (615) 790-2548 or the Nolensville office at (615) 941-1000.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
GLP-1 microdosing and maintenance dosing are physician-guided strategies, not internet shortcuts. Learn what each term means, why interest is growing, what the evidence shows, and
Once a GLP-1 medication quiets your appetite, knowing what to eat matters more than ever. This practical guide covers protein targets, the foods that worsen
Tirzepatide is available now for physician-supervised weight loss in Franklin and Nolensville, TN. Here is what the medication is, how local availability differs from telehealth

Retatrutide’s phase 2 trial produced an average of about 24% body weight loss, higher than the numbers seen with approved medications like tirzepatide and semaglutide.
Every few years a new weight-loss medication comes along that changes the conversation. Right now, that name is retatrutide. It has produced some of the
If you have been researching weight-loss medications, you have run into the same three names again and again: semaglutide, tirzepatide, and the newcomer everyone is