Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
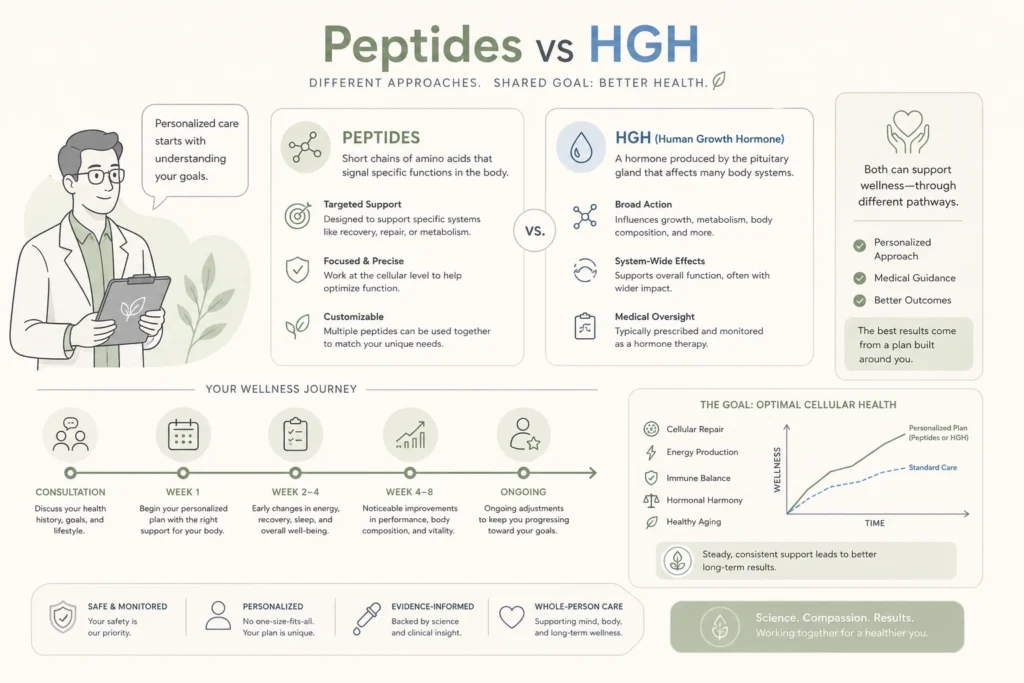
Most people walking into a peptide therapy consultation are quietly comparing two things in their head: the synthetic growth hormone an aging movie star reportedly used, and the peptide stack their friend posted about on social media. They sound similar. They are not.
The honest comparison of peptides vs HGH is not a horserace between two competing performance drugs. It is a comparison between a tightly regulated prescription hormone with serious risks at non-therapeutic doses, and a category of signaling molecules that nudge your own pituitary to do what it already does. Different mechanisms. Different regulation. Different risk profiles. Different candidates. At Body Works in Franklin, TN and Nolensville, TN, we walk patients through this comparison every week. Here is the version you can take home.
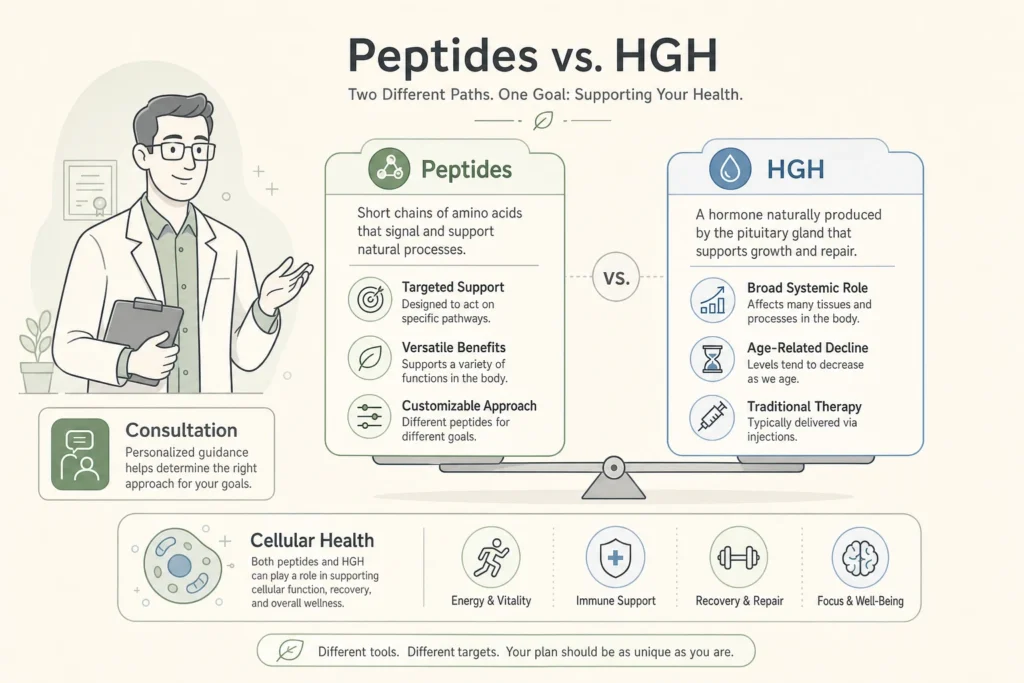
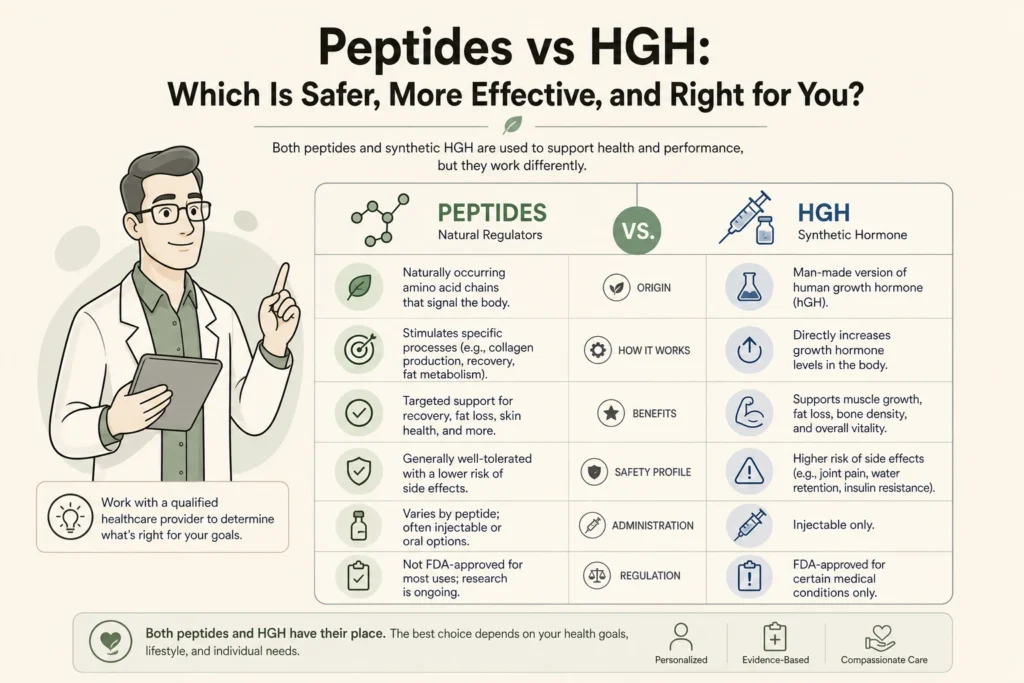
Synthetic human growth hormone, sold as somatropin, is recombinant DNA-produced human growth hormone given by daily subcutaneous injection. It replaces the hormone directly. Growth hormone releasing peptides like sermorelin, CJC-1295, and ipamorelin do not replace anything. They bind to receptors that prompt your pituitary gland to release its own growth hormone in a pulsatile pattern that mimics normal physiology.
That mechanism difference is the entire reason the safety profiles diverge. Synthetic HGH bypasses every feedback loop your body uses to keep growth hormone within range, which is why supraphysiologic dosing is possible and why the side effect list is long. Growth hormone releasing peptides work upstream of the pituitary, so when your body has had enough growth hormone for the day, negative feedback shuts the response down. Per the Endocrine Society’s Adult Growth Hormone Deficiency Clinical Practice Guideline, GH replacement is reserved for documented adult deficiency, not for general anti-aging or wellness goals.
Synthetic HGH is FDA approved for a narrow set of conditions. According to the FDA Import Alert 66-71 on unapproved human growth hormone, approved adult indications are limited to documented adult growth hormone deficiency and short bowel syndrome, while pediatric approvals cover specific genetic and growth conditions such as Turner syndrome and Prader-Willi syndrome. The same alert confirms that distributing HGH for anti-aging, athletic performance, or general wellness use falls outside FDA approval, and unapproved HGH products are subject to detention at the border.
Peptides have a different regulatory status. Sermorelin was once FDA approved for diagnosing pediatric growth hormone deficiency, then voluntarily withdrawn from the market in 2008. Today, sermorelin, CJC-1295, and ipamorelin are prescribed as compounded medications through 503A pharmacies. Per the FDA Bulk Drug Substances Compounding page, the FDA reviews each peptide on a case-by-case basis for inclusion on the 503A bulks list. Several peptides remain under active review. We tracked the April 2026 changes in our guide to the 2026 peptide regulatory shifts.
Supraphysiologic HGH dosing, the kind used outside FDA-approved indications, carries cardiometabolic and oncologic concerns. A review of growth hormone use and abuse in sport, published in Endocrine Reviews in 2019 explains that GH is a banned doping agent whose anabolic effects are largely mediated by IGF-1, the same axis implicated in cell proliferation. The FDA itself lists an increased risk of cancer among the long-term side effects of HGH. Long-term non-medical use is also associated with hypertension, cardiomyopathy, diabetes, and acromegaly, which is the irreversible thickening of the bones in the hands, feet, and jaw.
Growth hormone releasing peptides have a different profile because they do not override pituitary feedback. The most common side effects reported with sermorelin, CJC-1295, and ipamorelin are mild and transient: injection site redness, brief flushing, water retention, and occasional headaches in the first weeks. The pulsatile release pattern means peak GH and IGF-1 levels stay within or near physiologic range. Patients with active malignancy, severe diabetic retinopathy, or uncontrolled hypertension are still ruled out at the consultation stage, and ongoing bloodwork is the standard of care in any reputable program.
The table below summarizes how the two approaches differ across the dimensions that matter most to a patient deciding between them.
| Factor | Synthetic HGH (somatropin) | Growth Hormone Releasing Peptides (sermorelin, CJC-1295, ipamorelin) |
|---|---|---|
| Mechanism | Replaces growth hormone directly; bypasses pituitary feedback | Stimulates your own pituitary to release endogenous growth hormone in pulses |
| FDA Regulation | FDA approved for adult GH deficiency, short bowel syndrome, HIV wasting, and specific pediatric conditions only. Non-medical distribution illegal under federal law. | Compounded via 503A pharmacies with a physician prescription. Each peptide reviewed individually on the 503A bulks list. |
| Typical Side Effects | Fluid retention, joint pain, carpal tunnel, insulin resistance, edema; at supraphysiologic doses, hypertension, cardiomyopathy, acromegaly, and cancer-signaling concerns | Mild and transient: injection site reactions, brief flushing, mild water retention, occasional headache. Pulsatile release respects negative feedback. |
| Best Candidate | Adults with biochemically documented growth hormone deficiency confirmed by stimulation testing | Generally healthy adults seeking modest, physiologic support for sleep, recovery, body composition, or aging concerns, screened for contraindications |
| Realistic Results Timeline | Body composition shifts measurable at 3 to 6 months in true deficiency; lifelong replacement | Sleep changes in 2 to 4 weeks; body composition and recovery shifts at 8 to 12 weeks; cycled rather than indefinite |
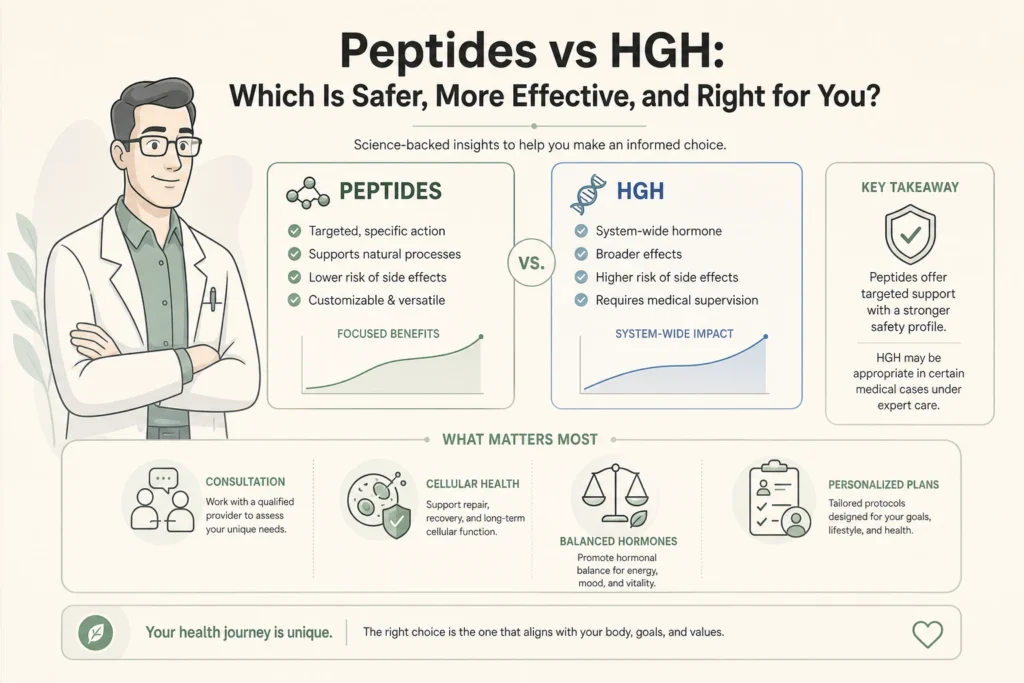
The decision is not really peptides vs HGH for most patients walking into a wellness consultation. The real decision is whether your situation meets the strict criteria for HGH replacement, or whether a growth hormone releasing peptide is a more proportionate fit for what you actually want.
HGH replacement is appropriate for adults with confirmed growth hormone deficiency from pituitary disease, traumatic brain injury, or other documented causes, diagnosed by stimulation testing rather than a single low IGF-1 reading. Per Molitch et al., Endocrine Society Clinical Practice Guideline, JCEM 2011, true adult GH deficiency benefits from replacement, but the diagnosis requires careful biochemical confirmation. For everyone else, growth hormone releasing peptides offer a more physiologic option. A landmark study by Teichman et al., JCEM 2006 showed that a single dose of CJC-1295 produced dose-dependent increases in plasma GH and 1.5 to 3 fold increases in IGF-1 lasting 9 to 11 days in healthy adults, demonstrating sustained physiologic stimulation rather than replacement.
Body Works does not prescribe synthetic HGH. We refer patients with suspected adult growth hormone deficiency to endocrinology for stimulation testing and replacement when indicated. What we offer at the Franklin and Nolensville clinics is physician-supervised peptide therapy, with bloodwork first, candidacy review, and ongoing monitoring on cycle. Patients also considering testosterone optimization can pair peptide protocols with our men’s hormone therapy program, since the two interventions support different biological pathways.
For a deeper look at the broader category, our complete guide to peptide therapy covers mechanism, indications, and what to ask a provider before you start. If you are newer to the topic, our plain-English peptide primer is the gentler starting point.
If you are weighing this comparison and want to know which path actually fits your bloodwork, history, and goals, the safest next step is a physician-supervised conversation. Schedule a Free Consultation at the Franklin or Nolensville location. Call the Franklin office at (615) 790-2548 or the Nolensville office at (615) 941-1000.
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
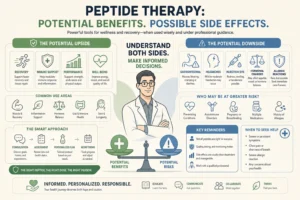
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never