If you are researching medical weight loss, two medication names keep coming up: semaglutide and tirzepatide. Both have changed what is possible with non-surgical weight loss, and there is now head-to-head clinical data showing how they stack up against each other. But they are not interchangeable, and the right choice depends on how each medication works, your medical history, and how your body responds during treatment.
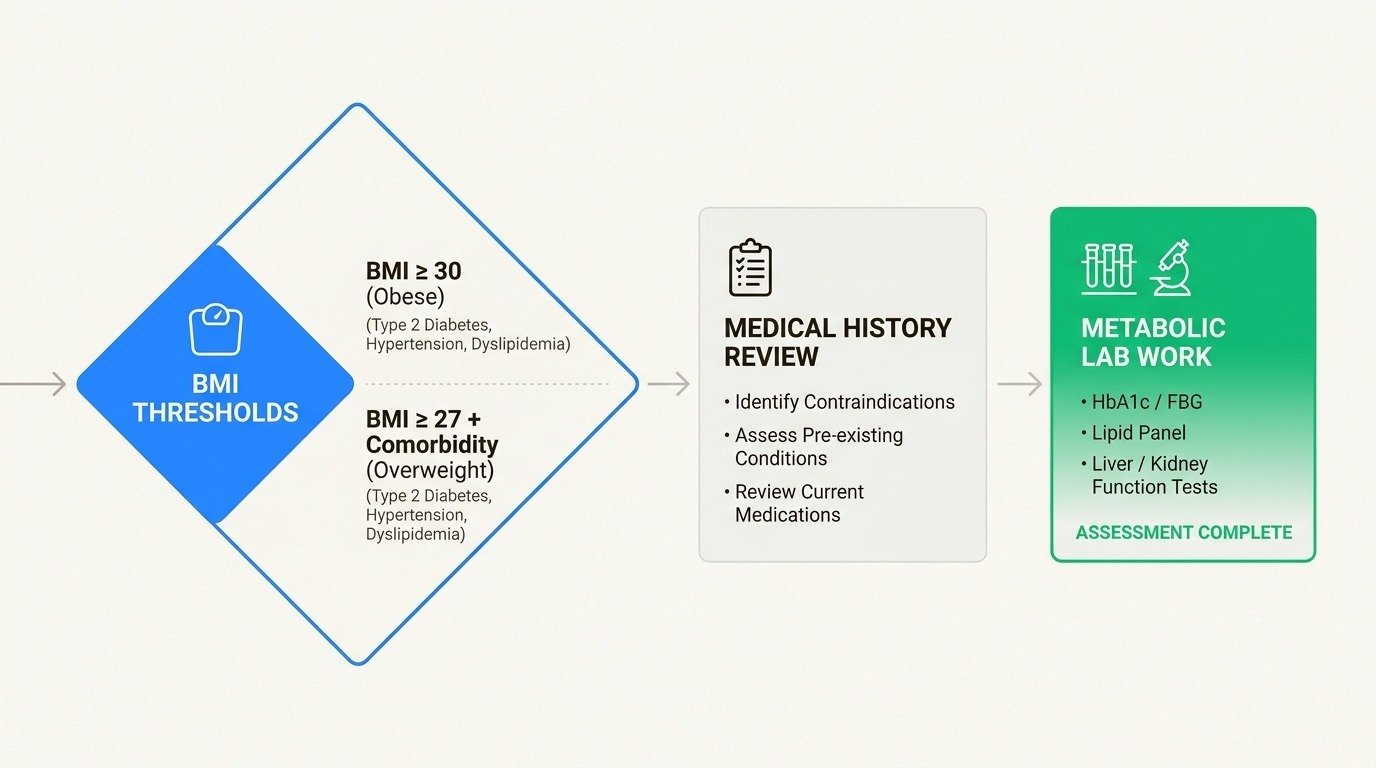
At Body Works in Franklin, TN and Nolensville, TN, physicians prescribe both semaglutide and tirzepatide and tailor the selection to each patient. According to the National Institute of Diabetes and Digestive and Kidney Diseases, GLP-1 receptor agonists now produce 3 to 12% more weight loss than lifestyle intervention alone. This guide walks through the latest clinical evidence, including the 2025 SURMOUNT-5 head-to-head trial, so you can have an informed conversation with your provider.
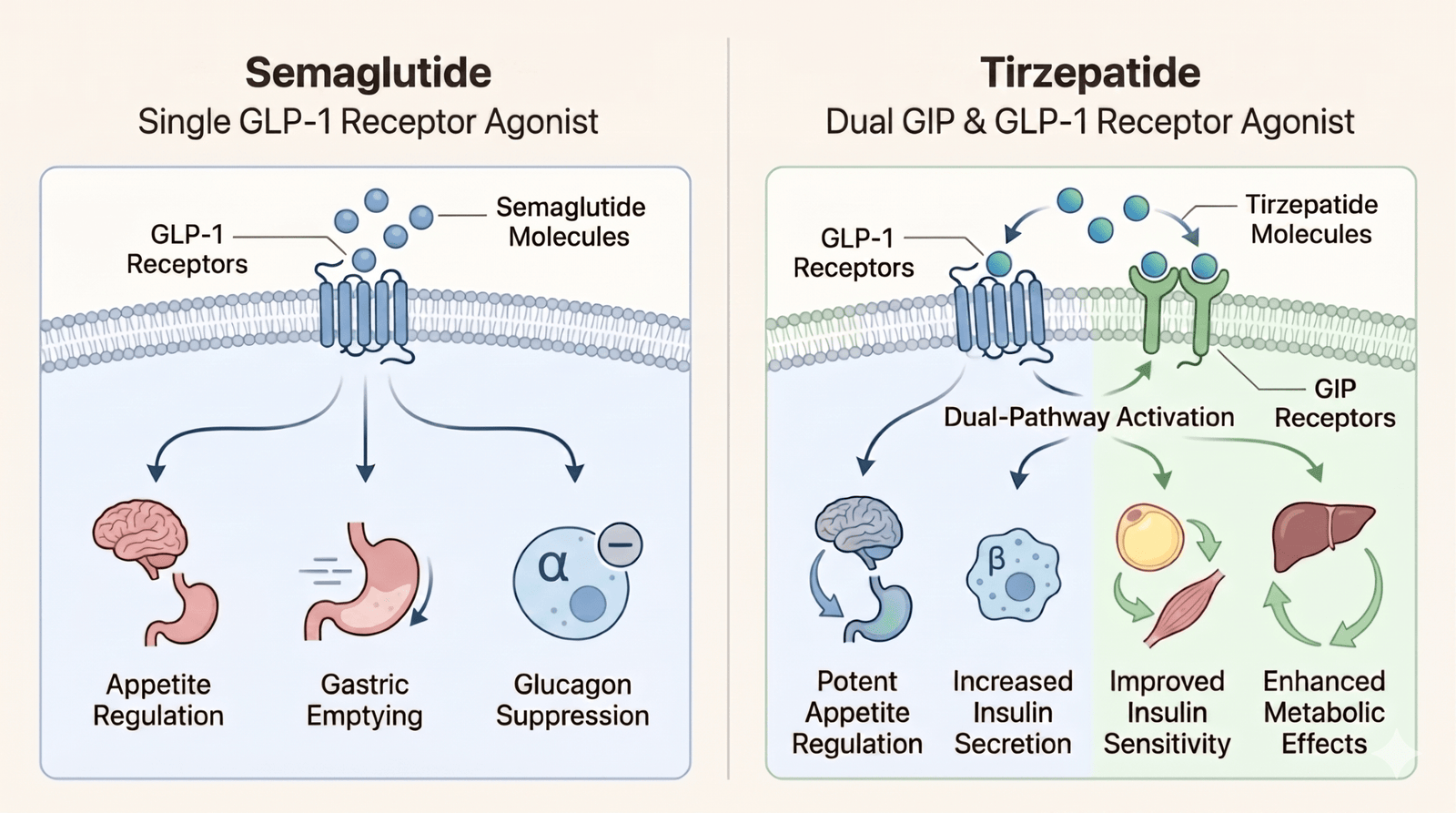
Both medications belong to a class called incretin mimetics, but tirzepatide engages a second hormone pathway that semaglutide does not. Semaglutide is a pure GLP-1 receptor agonist: it mimics glucagon-like peptide-1, a hormone your gut releases after eating. It acts on the appetite center in your hypothalamus, slows gastric emptying so food stays in your stomach longer, stimulates insulin release when blood sugar is elevated, and suppresses glucagon.
Tirzepatide is a dual GLP-1 and GIP receptor agonist. It activates the same GLP-1 pathway semaglutide uses, but it also targets glucose-dependent insulinotropic polypeptide (GIP) receptors. Researchers believe this dual action enhances insulin sensitivity and fat metabolism beyond what single-pathway GLP-1 treatment achieves, and may offer additional benefits for bone formation and kidney function.
Both medications are taken as once-weekly subcutaneous injections and work best alongside a reduced-calorie diet and regular physical activity. If this drug class is new to you, our primer on what GLP-1 medications are and how they work covers the fundamentals before the comparison details below.
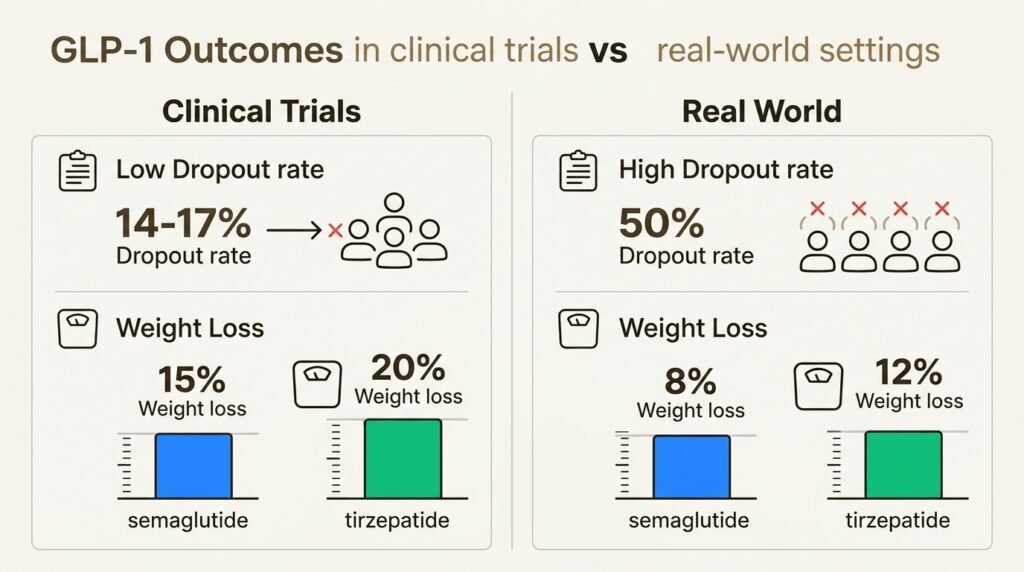
The SURMOUNT-5 trial, published in The New England Journal of Medicine in May 2025, is the first large randomized study to compare tirzepatide and semaglutide directly in adults with obesity. Over 72 weeks, tirzepatide produced notably greater weight loss across every metric the researchers measured.
| Outcome | Tirzepatide | Semaglutide | Difference |
|---|---|---|---|
| Mean body weight loss | -20.2% | -13.7% | -6.5 percentage points |
| Waist circumference reduction | -18.4 cm | -13.0 cm | -5.4 cm |
| Statistical significance | P<0.001 | P<0.001 | Highly significant |
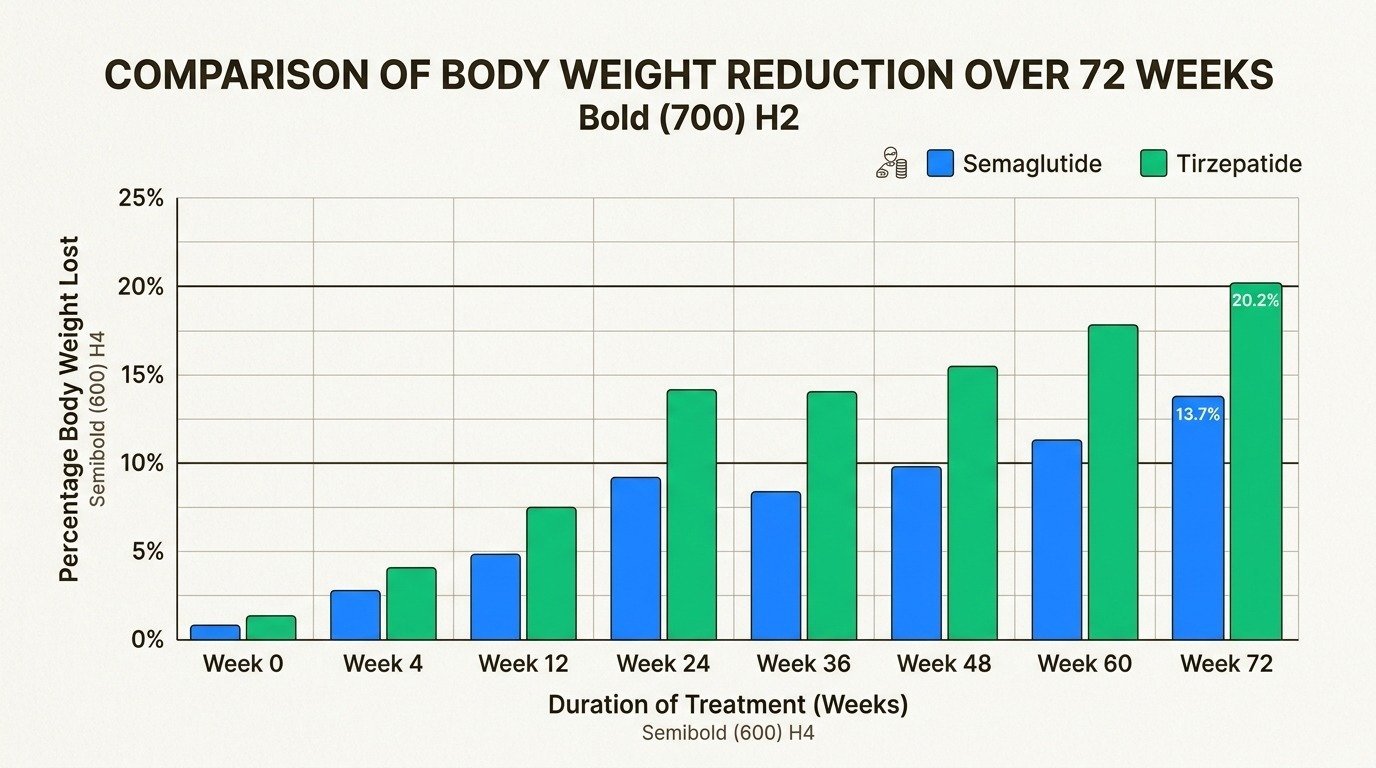
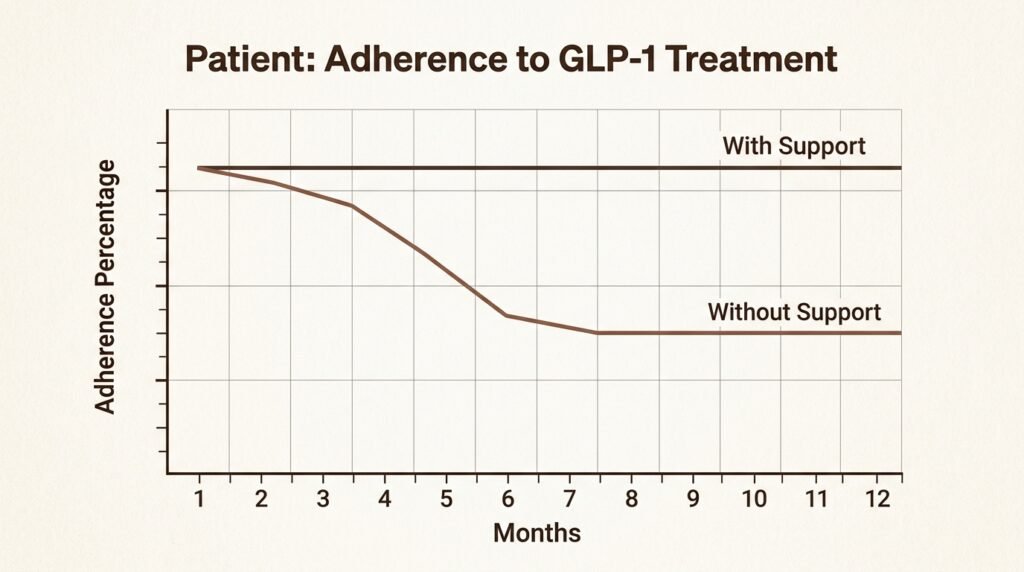
Significantly more tirzepatide patients hit every major weight loss milestone, including 10%, 15%, 20%, and 25% body weight reduction. Real-world data from electronic health records tells a similar story, though the gap narrows somewhat in patients who also have type 2 diabetes. These are averages, and individual results depend on starting weight, adherence to lifestyle changes, and metabolic factors. Our guide on how to succeed on medical weight loss injections walks through the habits that separate strong responders from weaker ones.
Semaglutide is available as a once-daily oral tablet, which is currently the only FDA-approved GLP-1 pill for weight management. Tirzepatide is injection-only. For patients who have significant needle anxiety or strongly prefer oral medications, this availability difference can be the deciding factor between the two classes.
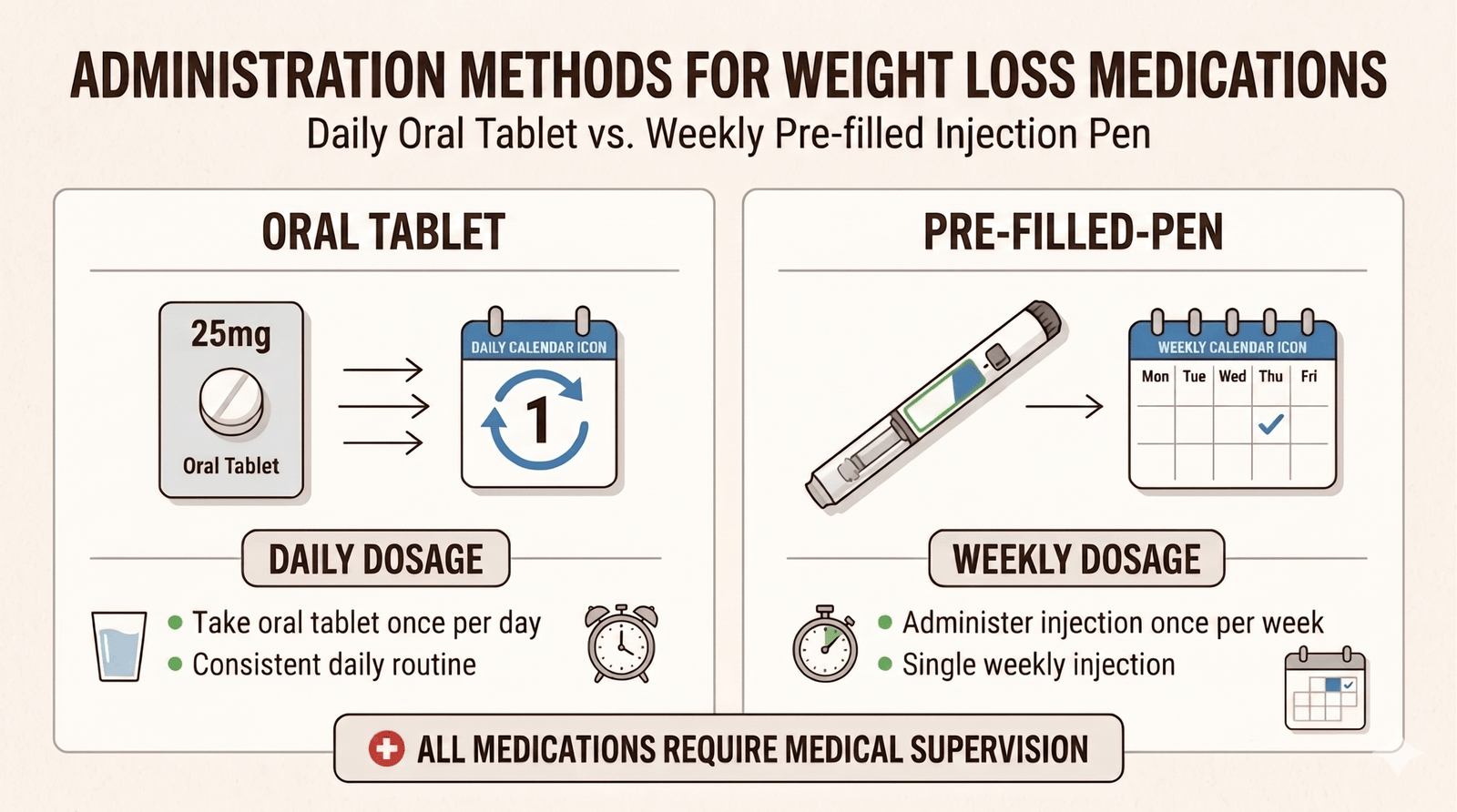
It is worth noting that the injectable forms are dosed once weekly, while the oral tablet is taken daily on an empty stomach with specific water and fasting instructions. Many patients find the weekly injection more convenient once they get past the initial apprehension about self-injection. Either route can work; the question is which fits your lifestyle and comfort level.
Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
Peptides and GLP-1 Weight Loss: Protecting Muscle and Skin
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
Tesamorelin for Visceral Fat: A Closer Look at Body Composition Peptides
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

Peptides for Active Adults: Recovery, Joint Health, and Longevity
If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
What Are the Side Effects of Peptide Therapy? An Honest Look
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

Peptides for Women Over 40: A Guide to Hormones, Energy, and Body Composition
You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never