Peptides and Testosterone Therapy: How They Work Together for Men’s Health
June 17, 2026
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads a forum, buys a vial of something labeled CJC-1295 online, and adds it to his testosterone on his own. That is the exact scenario a good physician spends an appointment talking patients out of.
The relationship between peptides and testosterone is real and useful, but it is widely misunderstood. Testosterone replacement therapy and growth hormone releasing peptides act on two different signaling systems in the body, which is precisely why some men benefit from coordinating both under one physician. They are two distinct medical therapies that share a monitoring plan, not a single stack you assemble from internet vials. At Body Works in Franklin, TN and Nolensville, TN, this is one of the more common conversations in a men’s health consultation. Here is how the two actually fit together.
How Do Peptides and Testosterone Work in Different Systems?
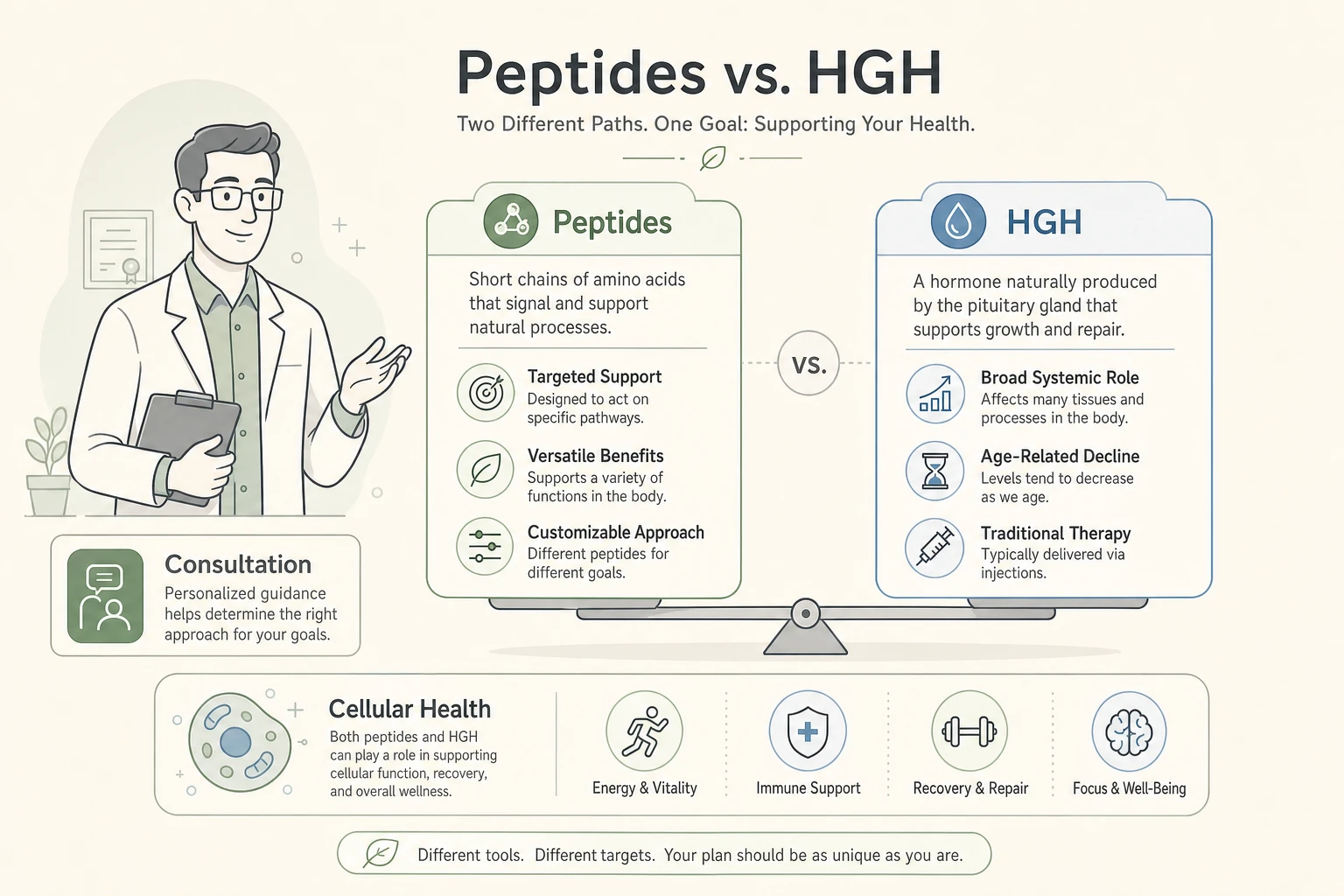
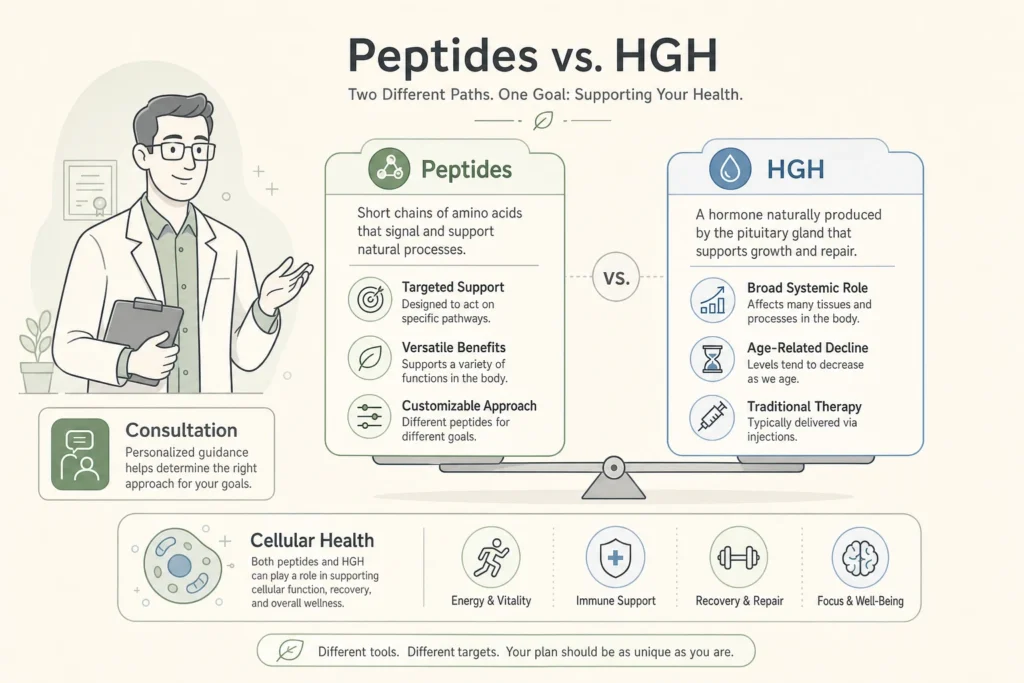
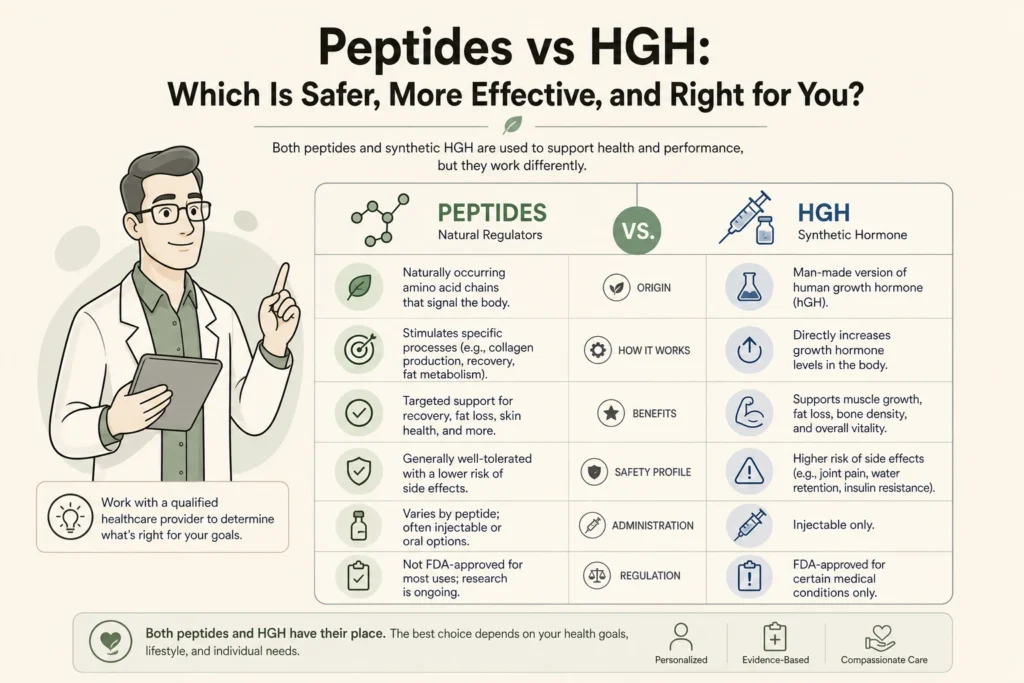
Testosterone and growth hormone releasing peptides act through two separate hormonal axes, which is why combining them under medical supervision can address complaints that testosterone alone does not fully resolve. Testosterone works through the androgen receptor to drive libido, red blood cell production, muscle protein synthesis, and mood. Growth hormone releasing peptides such as CJC-1295 and ipamorelin work upstream of the pituitary to prompt your own pulsatile release of growth hormone, which then raises IGF-1 and influences sleep depth, fat metabolism, and tissue repair.
Because the pathways are distinct, the symptoms they each touch are distinct. Testosterone deficiency review and the case for these as separable tools is laid out in a 2020 review in Translational Andrology and Urology on growth hormone secretagogues in hypogonadal males, which found that testosterone therapy reliably builds lean mass but that its effect on fat mass is often not significant, leaving a gap that growth hormone secretagogues may help close. That gap is the medical rationale for coordinating, not stacking blindly.
Why Do Some Men on TRT Add Growth Hormone Peptides?
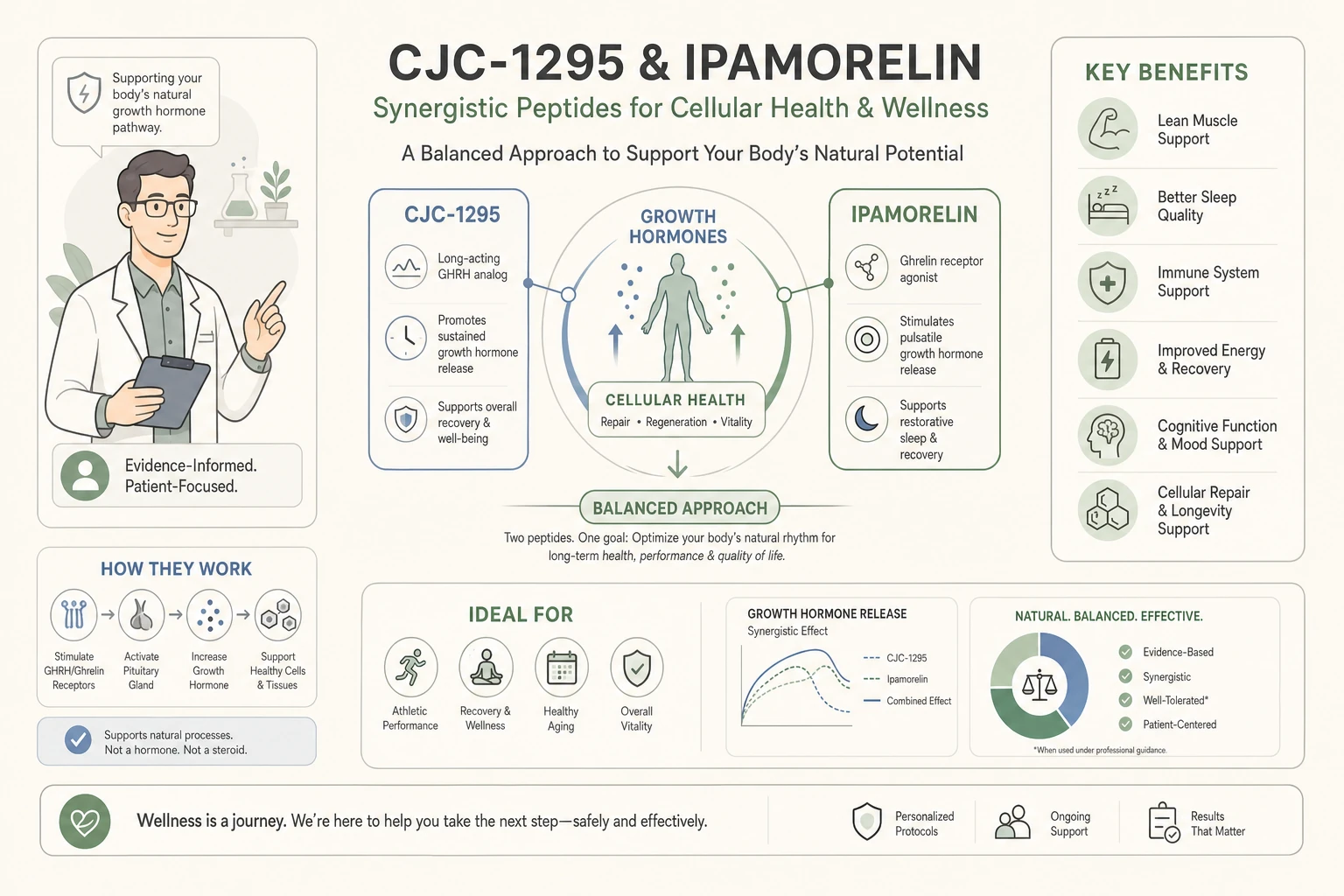
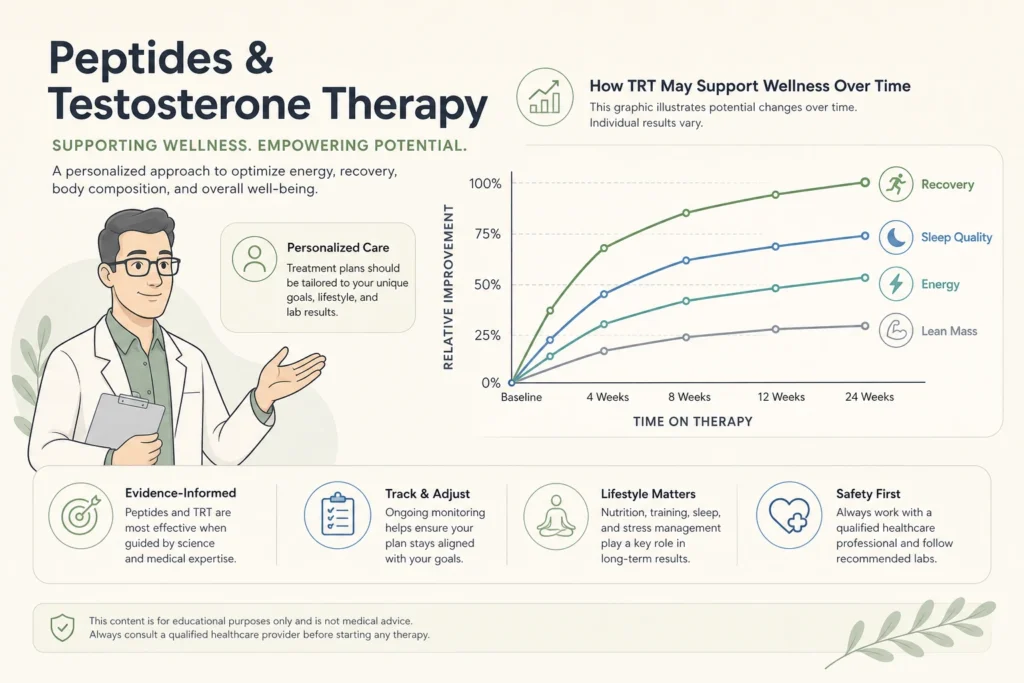
Men already on testosterone often add growth hormone releasing peptides because testosterone alone does not always restore sleep quality, recovery speed, or body composition to where they want it. Testosterone can rebuild muscle and drive, yet many men still report shallow sleep and slow recovery from training. Growth hormone is secreted largely during deep slow-wave sleep, and peptides like CJC-1295 paired with ipamorelin are used to support that nightly pulse.
The physiology behind this is documented. A study in Growth Hormone and IGF Research describing activation of the GH and IGF-1 axis by CJC-1295 reported that the long-acting GHRH analog raised growth hormone and produced sustained increases in IGF-1 in healthy adult men. Unlike injected synthetic growth hormone, this approach preserves the body’s pulsatile release pattern and its negative feedback, which is the safety distinction physicians care about. Patients curious about the specific protocol can read our deeper explainer on CJC-1295 and ipamorelin growth hormone peptides.
What Role Does BPC-157 Play During Heavier Training?
BPC-157 is used by some men as a connective-tissue support peptide when testosterone has improved their drive to train harder and joints and tendons start to feel the load. As men feel stronger on testosterone therapy, training volume tends to climb, and the soft tissue does not always keep pace. BPC-157 is a synthetic peptide studied for its effects on tendon, ligament, and muscle repair, and it is one reason recovery-focused patients ask about it.
The mechanism has an interesting tie to the growth hormone story. Research in the journal Molecules on BPC-157 and growth hormone receptor expression in tendon fibroblasts found that the peptide increased growth hormone receptor expression in tendon cells, which may sensitize healing tissue to the body’s own growth hormone. It is important to be candid here: most BPC-157 evidence is preclinical, human trials remain limited, and it is a compounded product that belongs under physician oversight, not in a self-directed regimen.
Why Is Bloodwork Monitoring Non-Negotiable Across Both Therapies?
Bloodwork is non-negotiable because testosterone and growth hormone peptides each move lab values that have to be watched together, and the overlap is exactly where unsupervised use becomes dangerous. Testosterone therapy raises hematocrit, the concentration of red blood cells, and an excessive rise increases the risk of clotting events. It also affects estradiol when testosterone converts to estrogen. Growth hormone peptides raise IGF-1, which should stay within an age-appropriate range rather than climbing unchecked.
The professional standard for testosterone monitoring is explicit. The Endocrine Society clinical practice guideline on testosterone therapy in men with hypogonadism recommends evaluating men after starting therapy for response, adverse effects, and adherence, and it flags a high hematocrit as a reason to withhold or stop treatment. A coordinated program checks testosterone, estradiol, hematocrit, and IGF-1 on a schedule, so a single physician sees the whole picture rather than two disconnected regimens drifting out of range.
Peptides and Testosterone: Distinct Therapies at a Glance
The table below shows why these are coordinated as separate therapies with a shared monitoring plan, not blended into one self-managed protocol.
| Factor | Testosterone Replacement Therapy | Growth Hormone Releasing Peptides |
|---|---|---|
| Primary pathway | Androgen receptor signaling | Pituitary growth hormone and IGF-1 axis |
| Main targets | Libido, muscle protein synthesis, mood, red blood cell production | Sleep depth, fat metabolism, tissue repair, recovery |
| Key labs to monitor | Total and free testosterone, estradiol, hematocrit, PSA | IGF-1, plus fasting glucose when relevant |
| Regulatory status | FDA-approved prescription therapy for documented hypogonadism | Compounded through 503A pharmacies under physician prescription |
| Why coordinate | Builds lean mass and drive, but may not fully resolve sleep or fat | Supports recovery and body composition gaps testosterone leaves open |
What Does Safe, Physician-Coordinated Care Look Like?
Safe care means one physician owns both therapies, orders the labs, sets the doses, and adjusts based on how your body responds, rather than you assembling a regimen from internet sources. Testosterone therapy itself has been reassured on the cardiovascular question by the TRAVERSE trial in the New England Journal of Medicine, which found testosterone noninferior to placebo for major adverse cardiac events in men with hypogonadism, while still noting a higher rate of certain arrhythmias. That is the kind of nuance a prescribing physician weighs; it is not something a forum thread can manage for you.
Peptides deserve the same rigor. A 2026 review in Frontiers in Aging on therapeutic peptides in gerontology describes peptides as targeted signaling molecules with mechanistically diverse effects, while drawing a clear line between agents with strong safety data and investigational compounds that still need validation. Coordinated care respects that line. To understand the regulatory picture for testosterone specifically, our explainer on the recent FDA stance changes on testosterone therapy is a useful companion read.
How Body Works Coordinates Peptides and Testosterone in Franklin and Nolensville
Body Works treats peptides and testosterone as two physician-managed therapies under one roof, starting with bloodwork and candidacy review before anything is prescribed. Men exploring testosterone optimization begin with our men’s hormone therapy program, which includes the baseline labs and follow-up testing the guidelines call for. When recovery, sleep, or body composition goals justify it, a physician-supervised peptide therapy plan can be added and monitored on the same schedule.
For men whose primary goal is fat loss alongside hormone optimization, our medical weight loss program can be coordinated into the same plan. If you want the full background before your visit, our complete guide to peptide therapy and our overview of how testosterone therapy works for men are good places to start.
The safest next step is a conversation with a physician who can read your labs and your goals together. Schedule a Free Consultation at the Franklin or Nolensville location. Call the Franklin office at (615) 790-2548 or the Nolensville office at (615) 941-1000.
Frequently Asked Questions
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
Browse Our Blog
Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
Peptides and GLP-1 Weight Loss: Protecting Muscle and Skin
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
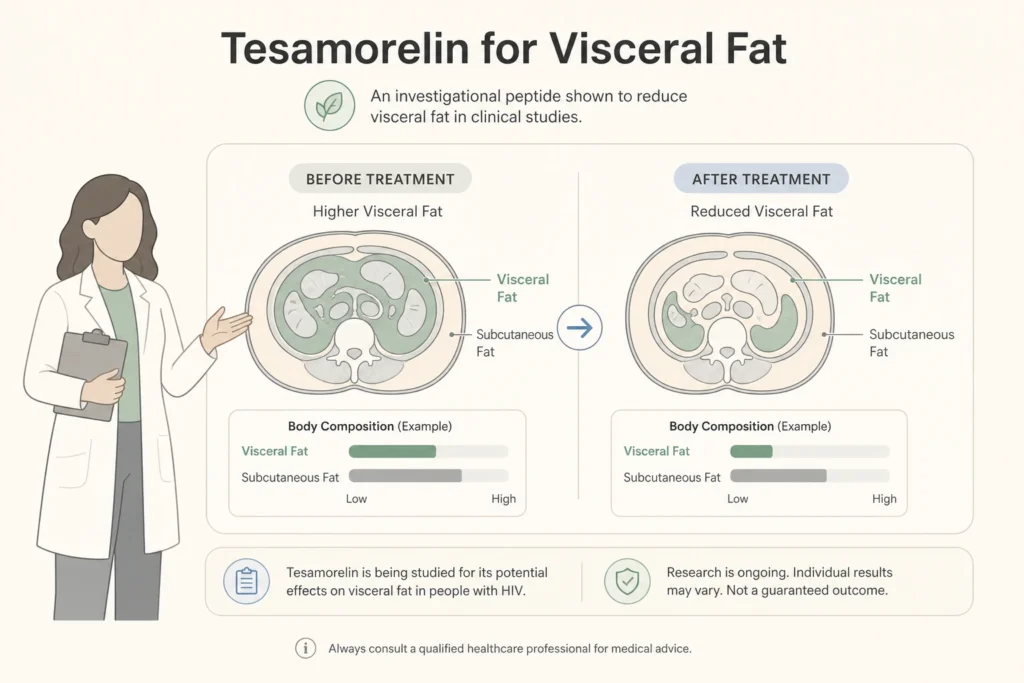
Tesamorelin for Visceral Fat: A Closer Look at Body Composition Peptides
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

Peptides for Active Adults: Recovery, Joint Health, and Longevity
If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
What Are the Side Effects of Peptide Therapy? An Honest Look
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

Peptides for Women Over 40: A Guide to Hormones, Energy, and Body Composition
You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never