Peptides for Better Sleep: How Growth Hormone Peptides Restore Deep-Wave Recovery
May 20, 2026
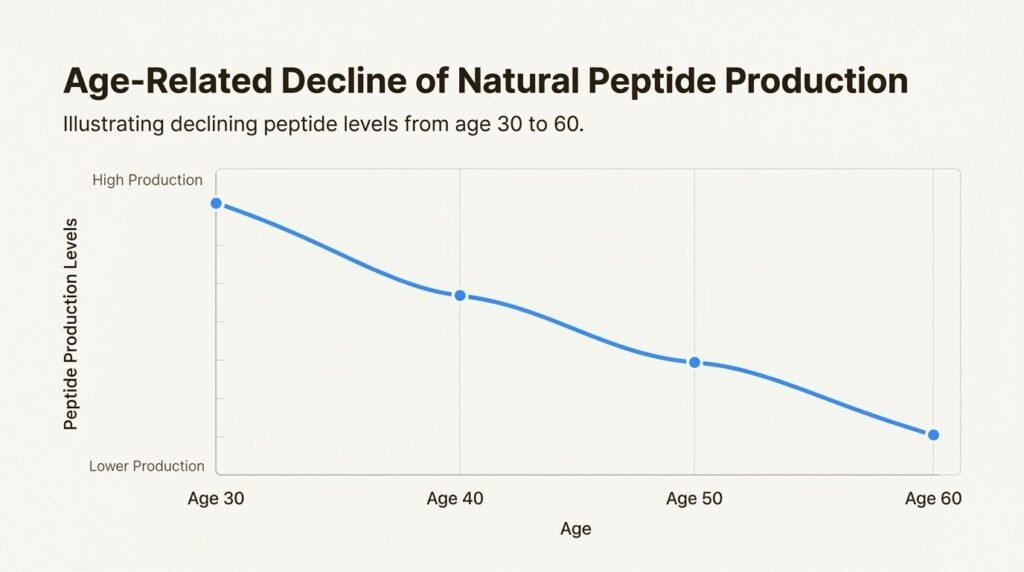
Sleep is not downtime. It is when tissue repair, immune restoration, and hormonal rebalancing happen. The problem is that the biology that drives deep sleep weakens with age. Growth hormone output during sleep falls steadily after the third decade. Deep slow-wave sleep, the most regenerative stage, shrinks from roughly a quarter of the night in young adults to under ten percent by the sixties. The fatigue and slow recovery many adults blame on stress is often the visible edge of that hormonal decline.
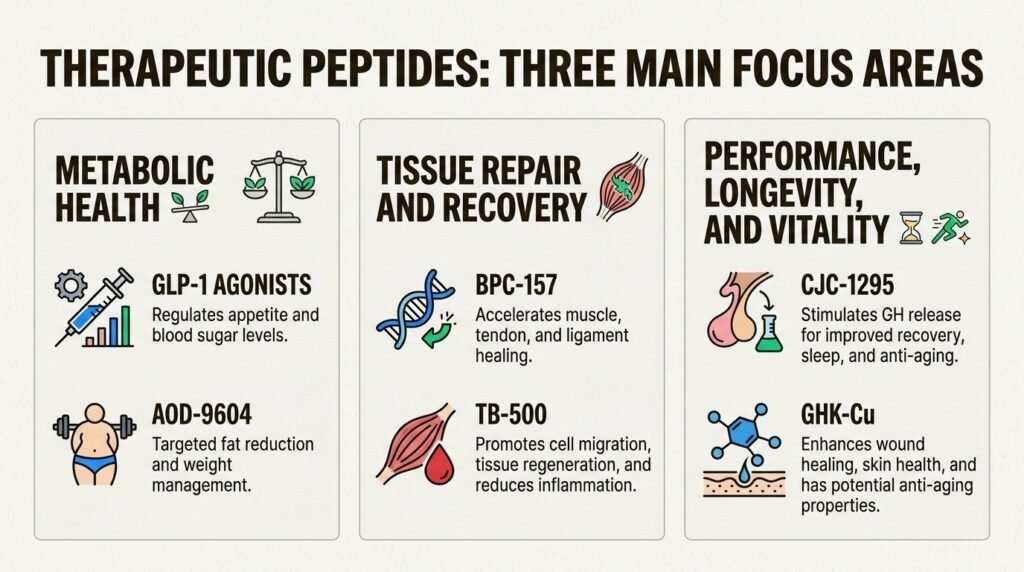
Growth-hormone-stimulating peptides like CJC-1295 and ipamorelin are one tool a physician-supervised program at Body Works in Franklin, TN and Nolensville, TN can use to support that biology. They do not sedate. They amplify the body’s own overnight growth hormone surge. This guide walks through how they work, what the peer-reviewed evidence actually shows, the realistic timeline, and where the limits are.

What Do Peptides Actually Do for Sleep?
Peptides are short chains of amino acids that function as signaling molecules. The peptides used for sleep optimization do not target sleep stages directly. They target the hormonal systems that govern sleep depth, especially the overnight pulse of growth hormone that drives slow-wave sleep. A classic study by Van Cauter and colleagues on age-related changes in slow-wave sleep and growth hormone, JAMA, 2000 showed that slow-wave sleep and growth hormone secretion decline together with age in healthy men, and that the two are tightly coupled across the night.
The practical reading: restoring even part of that overnight growth hormone signal can lengthen and deepen slow-wave sleep without changing total time in bed. Peptides that stimulate the pituitary to release more of the patient’s own growth hormone work upstream of the sleep stages themselves. They do not knock the brain out the way a benzodiazepine or a Z-drug does. They reinforce a biological signal the body is already trying to make.
How Does CJC-1295 Deepen Slow-Wave Sleep?
CJC-1295 is a synthetic analog of growth-hormone-releasing hormone (GHRH). It binds the GHRH receptor on the pituitary and prolongs the natural pulses of growth hormone release. A trial of CJC-1295 in healthy adults by Teichman and colleagues, a long-acting GHRH analog in healthy adults, Journal of Clinical Endocrinology and Metabolism, 2006 documented sustained increases in growth hormone and IGF-1 levels over multiple days after a single subcutaneous dose. The relevance for sleep is that growth hormone is released in pulses, and the largest pulse of the day occurs during the first few hours after sleep onset.
In a supervised protocol, CJC-1295 is typically injected in the evening so that its prolonged GHRH signal aligns with that early-night pulse. Most patients describe the change as feeling more “in” sleep rather than falling asleep faster. The first three to four hours of the night carry more weight, daytime fatigue eases, and morning grogginess decreases. The change is rarely dramatic in the first week and continues to build over four to eight weeks of consistent dosing.
How Does Ipamorelin Help With Sleep Onset?
Ipamorelin acts at a different receptor. It is a selective growth hormone secretagogue that binds the GHS-R (ghrelin) receptor on the pituitary to trigger a sharp, short pulse of growth hormone release. The original characterization by Raun and colleagues, ipamorelin as a selective growth hormone secretagogue, European Journal of Endocrinology, 1998 showed it releases growth hormone with minimal effect on cortisol, prolactin, or aldosterone, which is what makes it distinct from older GH-releasing peptides.
The clinical observation that follows is timing. Because the ipamorelin pulse peaks within thirty to sixty minutes, it can be dosed close to bedtime to put a GH spike on top of the body’s own first nocturnal pulse. Patients tend to notice the effect of ipamorelin earlier than CJC-1295: fewer mid-night awakenings, faster return to sleep after an awakening, and lighter morning grogginess. The deeper recovery effects on body composition and daytime energy follow over the same six-to-eight-week window as CJC-1295.
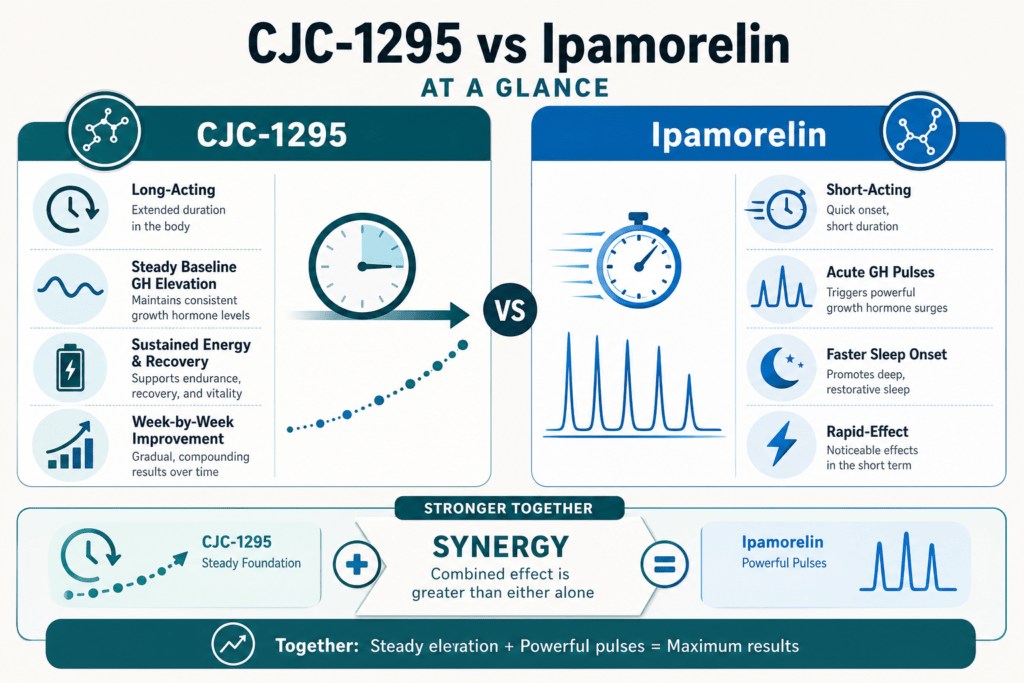
What Does Combining CJC-1295 and Ipamorelin Do?
The two peptides are often paired because they hit complementary parts of the same pathway. CJC-1295 stabilizes the underlying GHRH tone and raises the baseline of growth hormone release across the dosing window. Ipamorelin adds a sharper, acute pulse on top of that baseline through the ghrelin-receptor route. A peer-reviewed review by Sigalos and Pastuszak on growth hormone secretagogue safety and efficacy, Sexual Medicine Reviews, 2018 describes the GHRH-plus-secretagogue strategy and the literature on combined dosing.
In practice, supervised sleep-optimization protocols use the combination more often than either peptide alone. The combination requires the same baseline labs and the same physician oversight as either component on its own. It does not get prescribed casually, and it is not appropriate for every patient.
What Does the Research Actually Show About Peptides for Sleep?
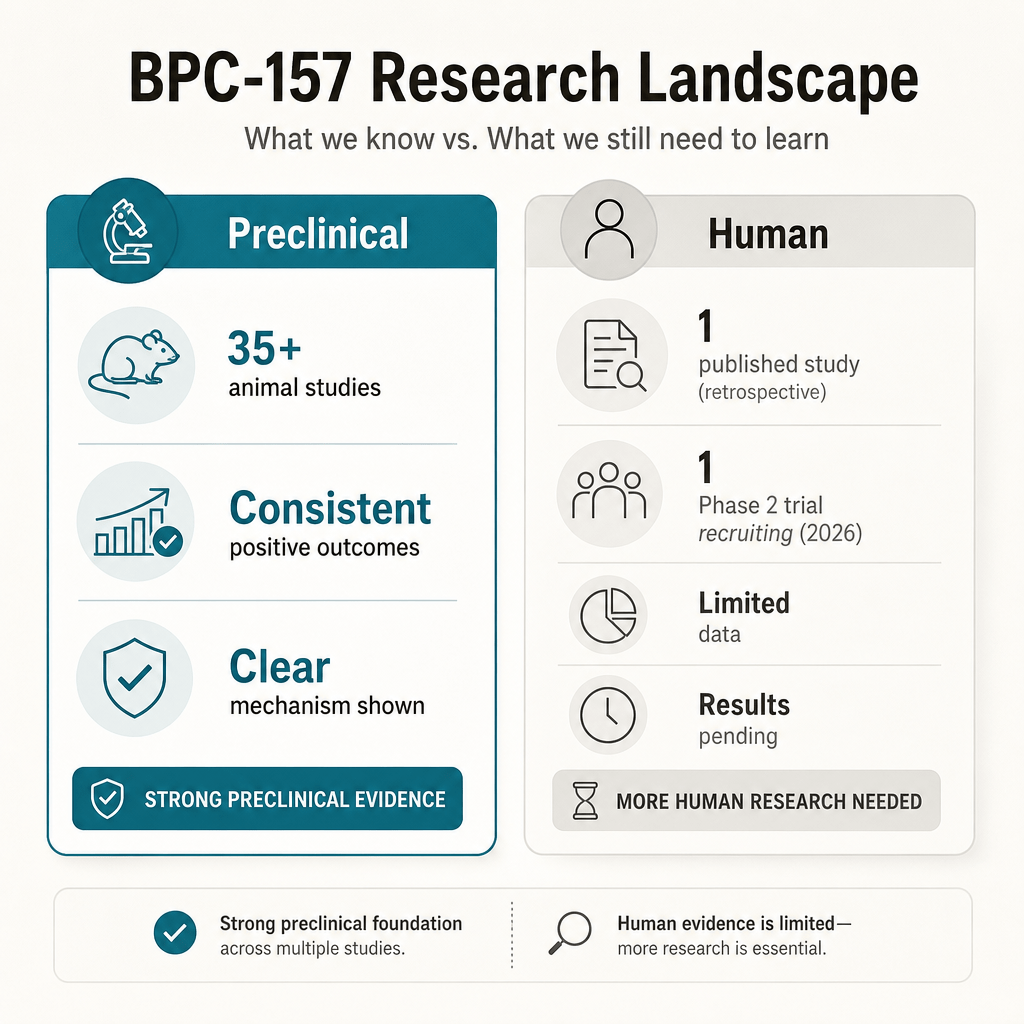
The honest framing matters. Growth hormone biology and sleep are well-studied in mechanism. The connection between slow-wave sleep, growth hormone release, and tissue recovery is established. CJC-1295 and ipamorelin each have human pharmacology data showing they raise growth hormone levels. What does not yet exist is a large, multi-year randomized trial of these specific peptides as a sleep treatment with overnight polysomnography as the primary endpoint.
That gap matters because patients evaluating peptide therapy deserve calibrated expectations. The mechanistic case is strong. The patient-reported outcomes inside supervised programs are encouraging. The randomized-trial-grade sleep data is partial. Endocrine Society clinical practice guidance on growth hormone therapy consistently emphasizes that newer compounds without large randomized trials require careful patient selection, baseline lab work, and ongoing monitoring rather than blanket use, and that framework is the right one for sleep-targeted peptide protocols too.
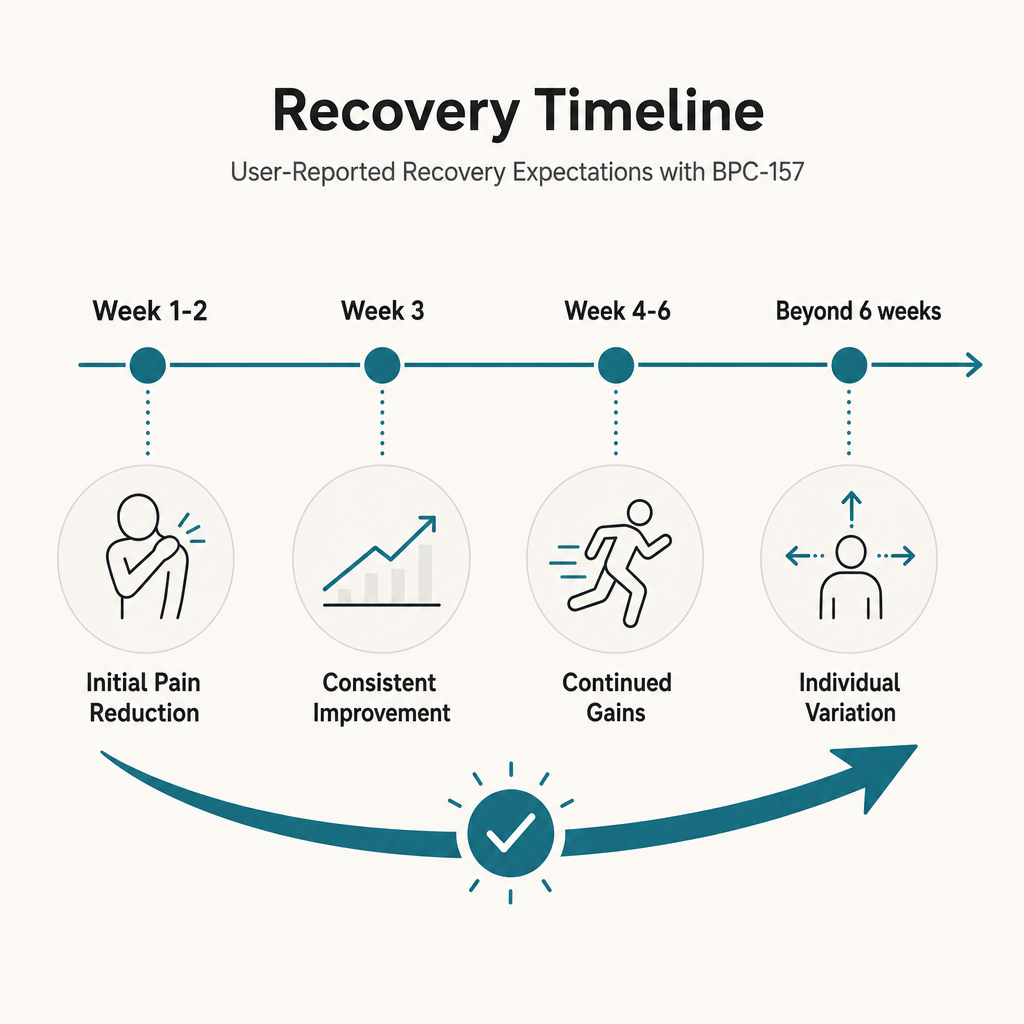
What Is the Realistic Timeline for Sleep Improvement?
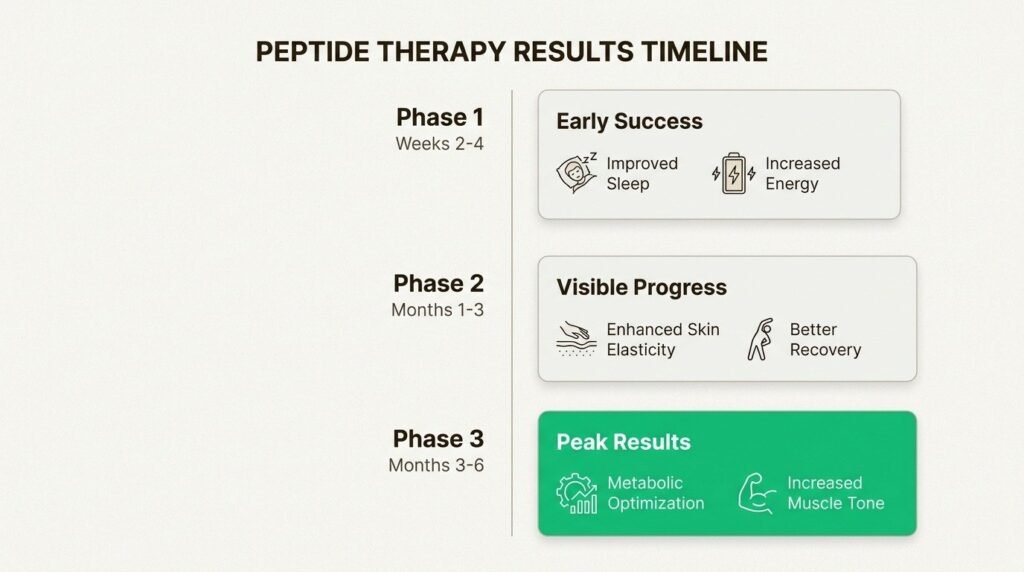
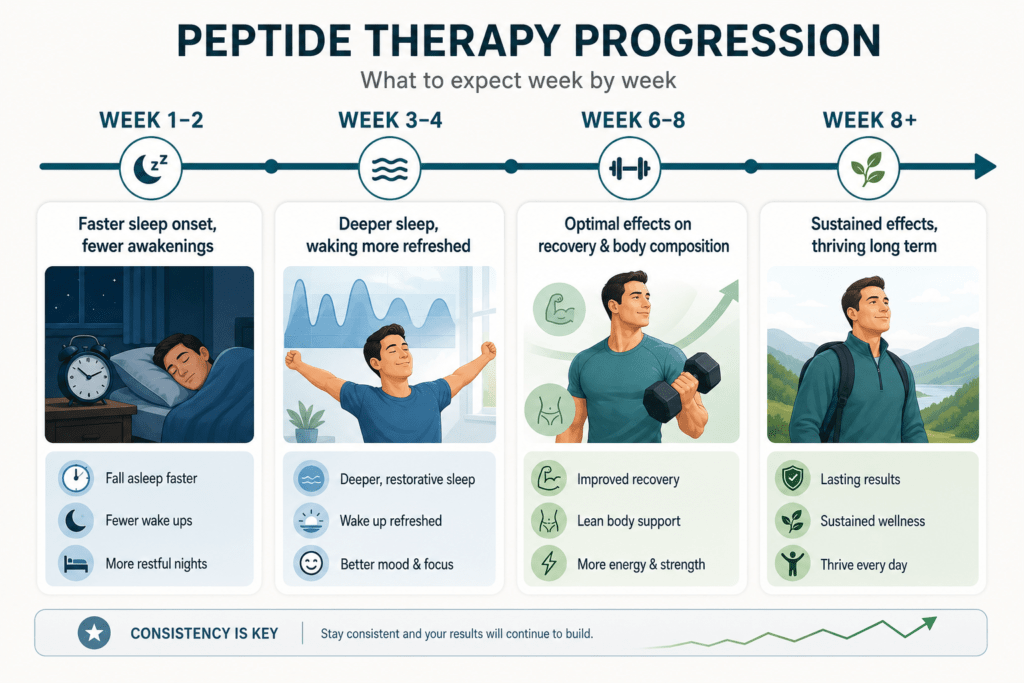
The pattern most supervised peptide patients report is steady rather than dramatic. In the first one to two weeks, the most common signal is faster sleep onset and fewer mid-night awakenings, especially with ipamorelin. By weeks three and four, slow-wave sleep starts feeling qualitatively different: morning waking is sharper, daytime energy stabilizes, and recovery from physical work improves. The full effect on body composition, lean muscle, and metabolic markers tends to emerge at the six-to-eight-week mark.
Several variables move the timeline. Patients who pair the peptide with consistent sleep timing, adequate protein, and structured exercise respond faster than patients who treat the peptide as a standalone fix. Patients with active inflammatory conditions, untreated thyroid issues, or significant nicotine and alcohol use tend to respond more slowly. Honest peptide programs are measured in months, not nights, and the patients who do best understand that.
Who Is a Reasonable Candidate for Sleep-Supporting Peptides?
The patients most often considered for CJC-1295, ipamorelin, or the combination in a physician-supervised program fall into a few groups. Adults in their forties through sixties dealing with the predictable age-related drop in growth hormone and slow-wave sleep. High-output professionals and active adults whose recovery has slowed even though training and sleep hygiene have not. Post-surgical patients trying to support overnight tissue repair without compromising standard recovery care. Patients with measurable IGF-1 or growth hormone deficits on baseline lab work.
The patients who are not appropriate candidates are equally important to name. Anyone with active malignancy or a recent history of it. Patients with uncontrolled diabetes or untreated pituitary disease. Pregnant or breastfeeding patients. Patients seeking a sedative or a sleeping pill replacement, which these peptides are not.
How Does Body Works Approach Peptide Therapy for Sleep?
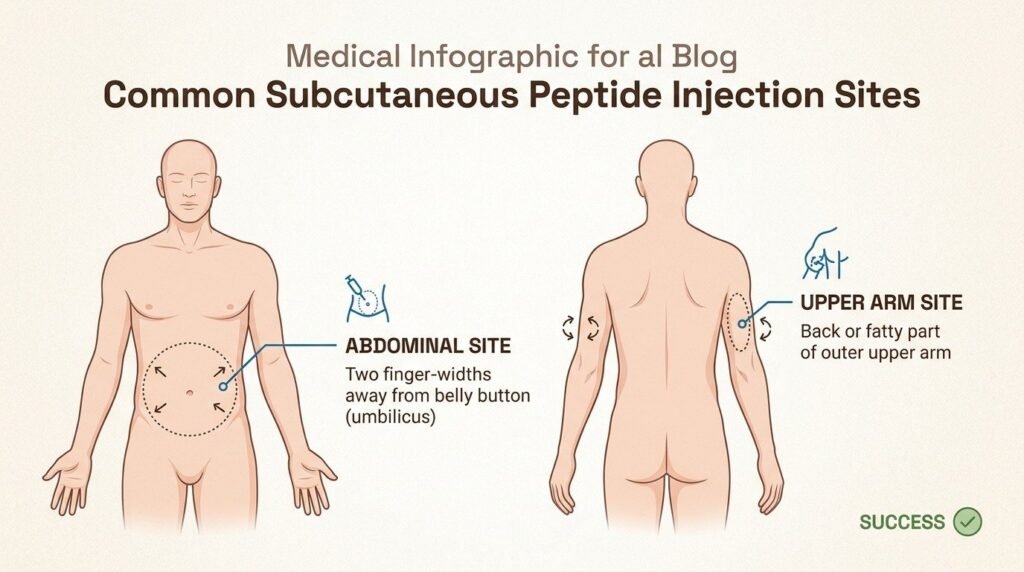
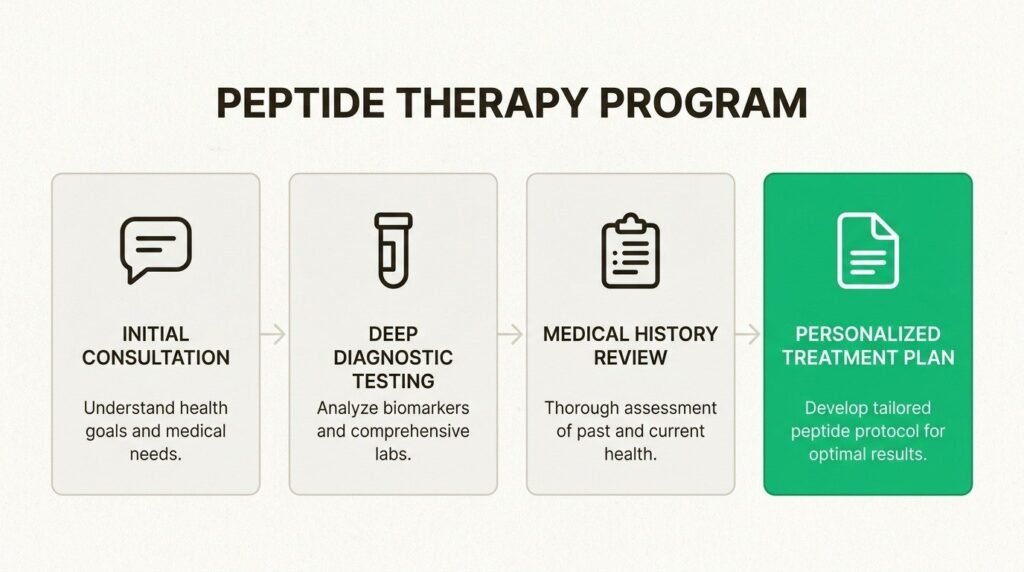
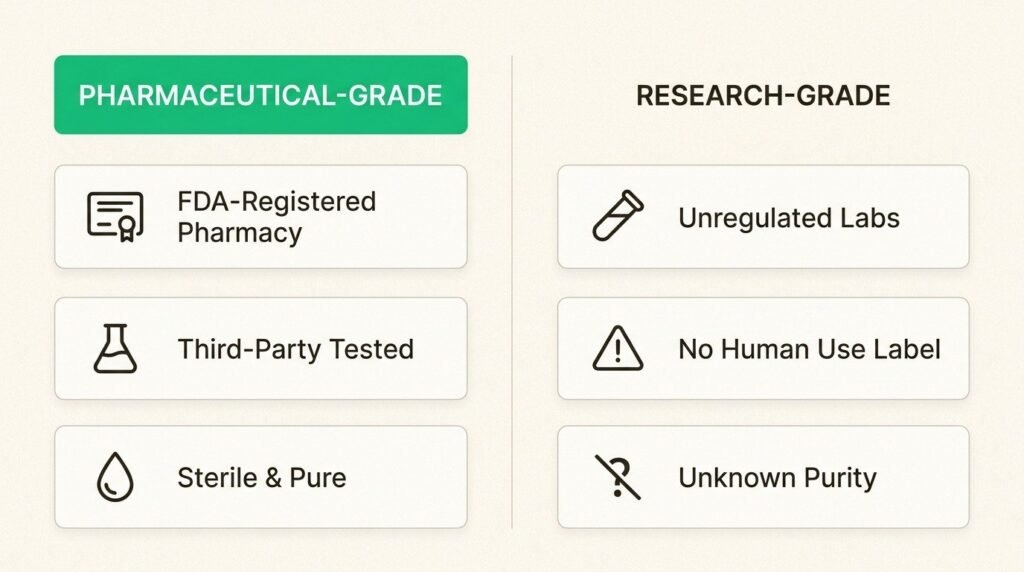
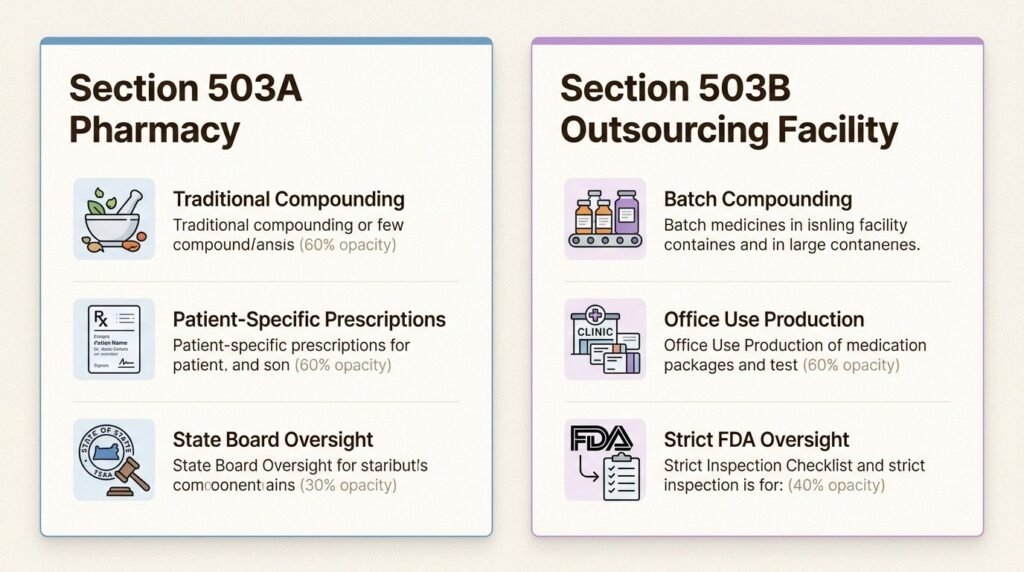
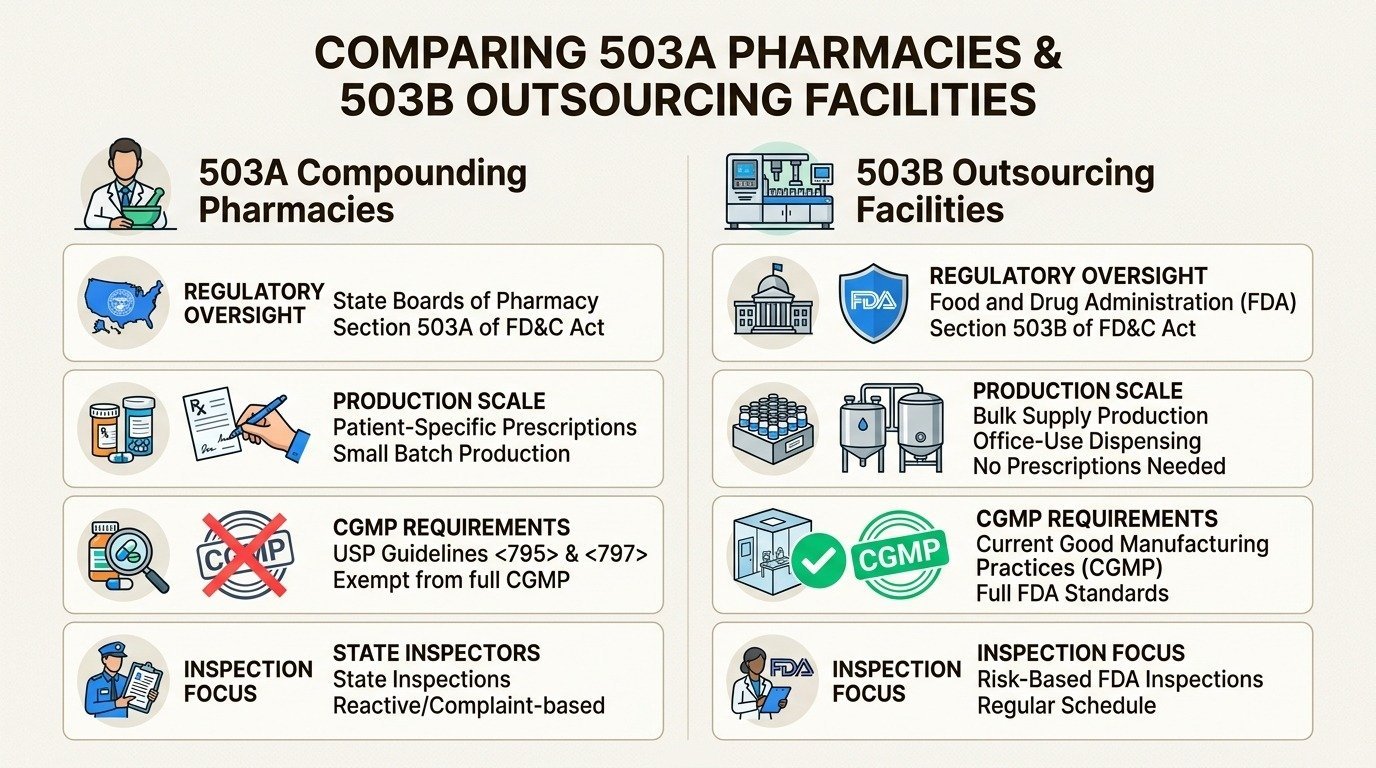
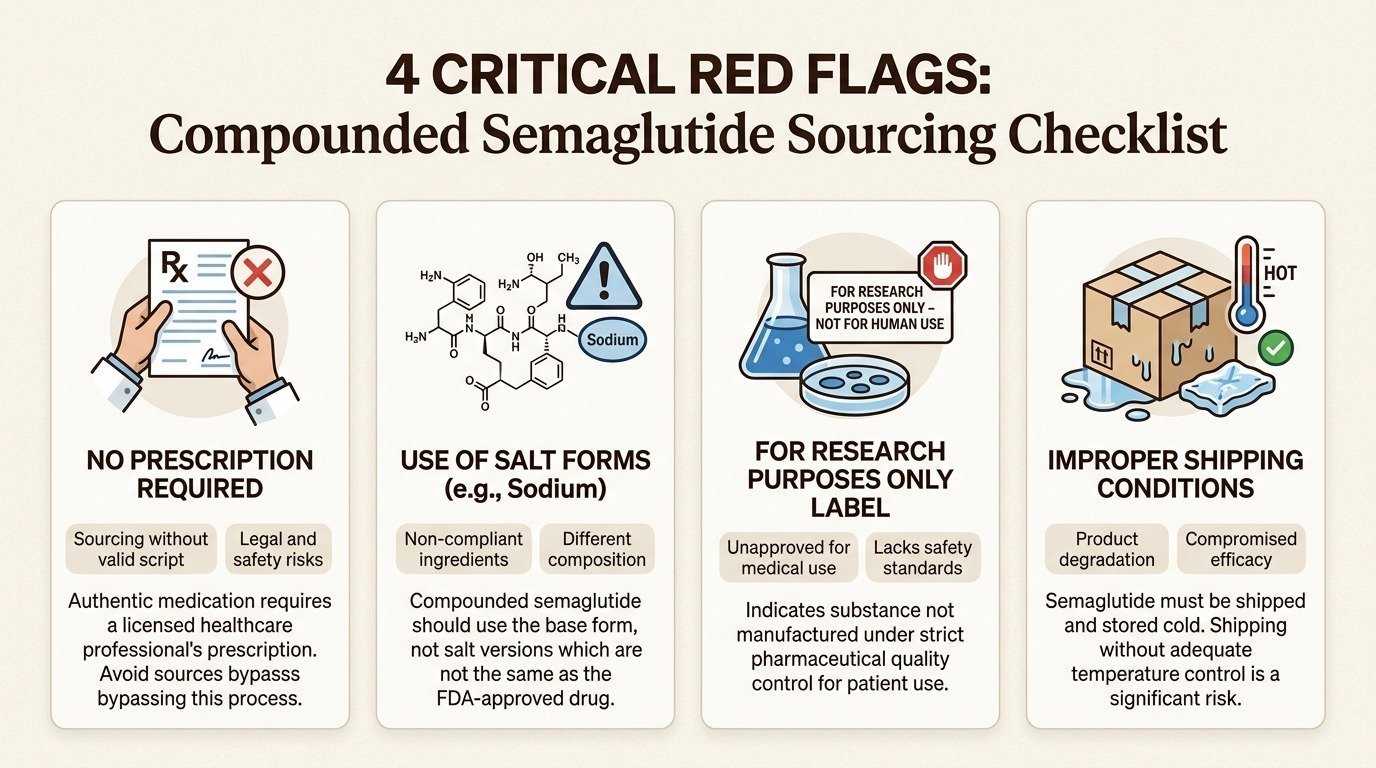
Sleep-targeted peptide therapy at Body Works sits inside the same structured framework as the rest of the peptide program. A consultation reviews goals, current medications, prior diagnoses, and any oncology or autoimmune flags. Baseline lab work includes IGF-1, growth hormone markers, fasting glucose, a metabolic panel, and thyroid markers when indicated. If a peptide protocol is appropriate, sourcing comes from accredited 503A compounding pharmacies, dosing is structured for the patient, and follow-up labs check both response and safety on a defined cadence.
A useful companion read is the existing post on peptide authenticity and sourcing, which covers what to look for in a 503A compounder. New readers can start with the plain-English guide to peptides, and the full category overview lives in the complete guide to peptide therapy.
What Should You Do Before Starting a Sleep-Peptide Protocol?
The right next step is a consultation, not a checkout. Peptides for sleep are not a supplement, and the patients who get the most out of them treat them as a medical decision rather than a wellness purchase. A physician-supervised peptide therapy program at Body Works in Franklin and Nolensville includes the candidacy review, baseline labs, sourcing oversight, dosing structure, and the follow-up that the published growth hormone literature recommends.
If poor sleep, slow recovery, or persistent daytime fatigue has you researching peptides, the most useful thing you can do is talk to a physician who works with this category. Schedule a Free Consultation with the Body Works team. You can reach the Franklin office at (615) 790-2548 or the Nolensville office at (615) 941-1000.
Frequently Asked Questions
Medically reviewed by Dr. Donald Vollmer, MD
Managing Physician, Body Works TN
Browse Our Blog
Peptides and Testosterone Therapy: How They Work Together for Men’s Health
A man starts testosterone therapy, feels better for a few months, then notices the recovery and sleep he expected never fully arrived. So he reads
Peptides and GLP-1 Weight Loss: Protecting Muscle and Skin
The number on the scale is dropping faster than it ever has. That is the promise of peptides and GLP-1 weight loss working together, and
Tesamorelin for Visceral Fat: A Closer Look at Body Composition Peptides
If you have spent any time reading about body composition peptides, you have probably run into a claim that one of them can melt the

Peptides for Active Adults: Recovery, Joint Health, and Longevity
If you are an active adult in your 40s or 50s, you have probably noticed that your ambition is still outrunning your body. The Saturday
What Are the Side Effects of Peptide Therapy? An Honest Look
If you have looked into peptide therapy side effects, you have probably found two extremes online: glowing testimonials that promise more energy and better skin

Peptides for Women Over 40: A Guide to Hormones, Energy, and Body Composition
You did not get lazy at 40. Two of your body’s main signaling systems quietly lost volume at the same time, and most women never